




DOES THE AFFORDABLE CARE ACT AFFECT PREVENTIVE CARE AMONG YOUNG ADULTS?

Department of Economics, Boston University, USA.
ABSTRACT
In this paper, I mainly focus on a provision in the Affordable Care Act (ACA), and this provision is that dependents whose age is up to 26 can be covered by their parents’ health insurance. On the basis of this provision in the ACA, I put forward my research question, which is whether the Affordable Care Act affects preventive care among young adults? To examine the research question, I choose Linear Probability Model within difference in difference as my main method. However, in the model regression, the coefficients of the interaction terms on flu shot and HIV Test are statistically insignificant, the results imply that the ACA does not affect the use of flu shot and HIV Test among young adults. As a common preventive care, the using of flu shot increases year by year, and it means young adults gradually raise healthy awareness. The using of HIV Test decreases year by year. Perhaps, HIV Test is not a common preventive care, and it is just for young adults who really need to take HIV Test.
Keywords:The ACA, Preventive care, Young adults, Flu shot, HIV Test, Difference-in-difference.
ARTICLE HISTORY: Received:7 June 2019 Revised:22 July 2019 Accepted:27 August 2019 Published:2 October 2019.
Contribution/ Originality:This study contributes in the existing literature related to the ACA and preventive care. Actually, this paper applies the linear probability model (LPM) within difference-in-difference to find out whether the ACA affects the use of preventive care among young adults.
1. INTRODUCTION
The Affordable Care Act (ACA) is to reform the health care system in the United States. With long consultations and discussions, the ACA was enacted on March 23, 2010. The ACA is designed to improve health insurance and expand Medicaid eligibility to reduce the number of uninsured people. The main goals of the Affordable Care Act are to minimize the number of uninsured Americans and make health care available to everyone at an affordable price (Coffin and Rak, 2013![]() ). After the ACA, the number of uninsured people gradually decreased (Carman et al., 2015
). After the ACA, the number of uninsured people gradually decreased (Carman et al., 2015![]() ). Because the cost of preventive cares can be covered by the insurance, more and more insured people may receive preventive care and keep healthy. Many provisions in the ACA are aimed at improving health insurance and expanding coverage to uninsured group. For example, some provisions mandate that providing more preventive care without co-pays and deductible, or the government needs to pay more for Medicaid, CHIP, and subsidy to those with low incomes who purchase through Health Insurance. The ACA expands eligibility for people to apply Medicaid or enlarges health insurance coverage, and expanding Medicaid eligibility or health insurance coverage has influence on health insurance related to health care (Finkelstein et al., 2012
). Because the cost of preventive cares can be covered by the insurance, more and more insured people may receive preventive care and keep healthy. Many provisions in the ACA are aimed at improving health insurance and expanding coverage to uninsured group. For example, some provisions mandate that providing more preventive care without co-pays and deductible, or the government needs to pay more for Medicaid, CHIP, and subsidy to those with low incomes who purchase through Health Insurance. The ACA expands eligibility for people to apply Medicaid or enlarges health insurance coverage, and expanding Medicaid eligibility or health insurance coverage has influence on health insurance related to health care (Finkelstein et al., 2012![]() ). Besides, health insurance coverage for preventive care increases the utilization of recommended preventive care (Faulkner and Schauffler, 1997
). Besides, health insurance coverage for preventive care increases the utilization of recommended preventive care (Faulkner and Schauffler, 1997![]() ). In other words, expanding eligibility in health insurance coverage improves receipt of more types of preventive care services. Therefore, the ACA could have influences on preventive care.
). In other words, expanding eligibility in health insurance coverage improves receipt of more types of preventive care services. Therefore, the ACA could have influences on preventive care.
In this paper, I mainly focus on the utilization of preventive care among young adults, considering those whose age are 18-25 years old as young adults. There is a provision for young adults in the ACA, and this provision in the ACA is that dependents whose age are over 26-year-old cannot be covered under their parents’ health insurance plan. Before the ACA, maybe few young adults care about the use of health care, after the ACA, the provision improves uninsured young adults in health insurance coverage, so that the ACA may increase young adults’ utilization in preventive care. Because of the provision, the ACA expands insurance coverage for young adults and improves access to preventive care. Consequently, my research question is to examine whether the ACA really affects the demand for preventive care among young adults. In Figure 1 and Figure 2, they display that the percentage of using flu shot among young adults and slight older adults increases year by year, but the percentage of using HIV Test among young adults and slight older adults decreases after 2010. In Figure 1 and Figure 2, the line of young adults (treatment group) is almost parallel to the line of slight older adults (control group) before the ACA, so these two lines in Figure 1 and Figure 2 exist the parallel trends before the ACA. However, after the ACA, these two lines in Figure 1 and Figure 2 are not parallel to each other. That is, the two lines in Figure 1 and Figure 2 have not the common trends. Perhaps, the ACA stimulates the use of preventive care among young adults. To examine my research question, I prefer to utilize D-i-D to test the use of preventive care among young adults affected by the ACA. Since the dependent variable is binary variable, the best choice is probit or logit model. However, standard software cannot calculate the ‘correct’ standard error and magnitude of the interaction term in probit or logit model within difference in difference (Ai and Norton, 2003![]() ) . Finally, I incorporate the D-i-D technique in the Linear Probability Model (LPM). In my research question and method, I set up age group 18 – 25 years old as the treatment group and set up 27 – 34 years old as the control group. Because dependents up to age 26 can be covered under their parents’ private health insurance plan, adults whose age are between 27 years old and 34 years old cannot be covered their parents’ health insurance plan. In my paper, the topic is about preventive care. Because of the impact of the ACA on health insurance, and insurance coverage is expanded, more and more uninsured people have opportunity to be covered by their parents’ health insurance. The connection between the ACA and insurance coverage could access to improve the demand for health care or preventive care. Besides, the definition of preventive care is to decrease the rate of occurrence or incidence of diseases and provide a way for reducing or eliminating disease. In my opinion, preventive care is also an essential method to protect people or public health. Therefore, I choose preventive care to analyze whether it is affected by the provision in the ACA.
) . Finally, I incorporate the D-i-D technique in the Linear Probability Model (LPM). In my research question and method, I set up age group 18 – 25 years old as the treatment group and set up 27 – 34 years old as the control group. Because dependents up to age 26 can be covered under their parents’ private health insurance plan, adults whose age are between 27 years old and 34 years old cannot be covered their parents’ health insurance plan. In my paper, the topic is about preventive care. Because of the impact of the ACA on health insurance, and insurance coverage is expanded, more and more uninsured people have opportunity to be covered by their parents’ health insurance. The connection between the ACA and insurance coverage could access to improve the demand for health care or preventive care. Besides, the definition of preventive care is to decrease the rate of occurrence or incidence of diseases and provide a way for reducing or eliminating disease. In my opinion, preventive care is also an essential method to protect people or public health. Therefore, I choose preventive care to analyze whether it is affected by the provision in the ACA.
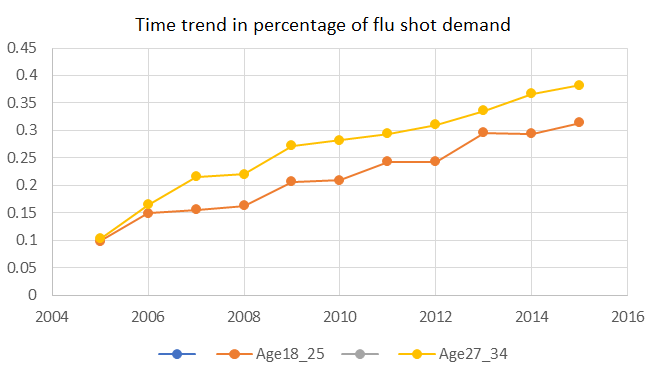
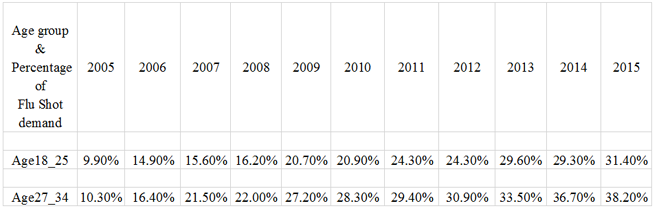
Figure-1. Trends in pre the ACA vs. post the ACA on Flu shot.
Source: The author’s own summary from the data in national health interview survey.
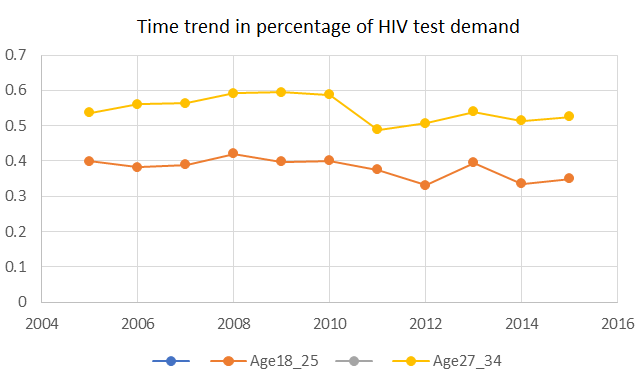
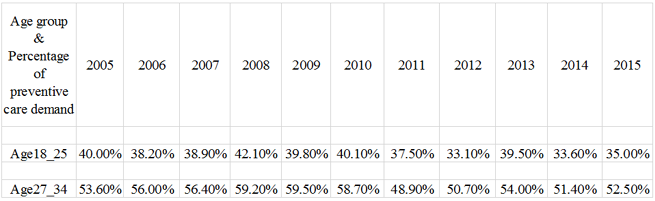
Figure-2. Trends in pre the ACA vs. post the ACA on HIV Test.
Source: The author’s own summary from the data in national health interview survey.
In general, the common preventive cares are wellness checks, immunization, and screenings. As we all know, infectious diseases still threaten public health. There are some negative results of Infection: 1) illness, 2) disability, 3) death in individual, 4) disrupting whole society. Vaccination is a sort of medical care to help public health prevent the spread of infectious and potentially deadly diseases (Institute of Medicine (U. S.), 2010![]() ). The flu shot is a sort of vaccination, so the flu shot can be regarded as one of preventive care, and HIV test is a routine preventive care for people who are potentially affected by HIV infection. Thus, I choose flu vaccinate and HIV test as main preventive care for studying in this paper.
). The flu shot is a sort of vaccination, so the flu shot can be regarded as one of preventive care, and HIV test is a routine preventive care for people who are potentially affected by HIV infection. Thus, I choose flu vaccinate and HIV test as main preventive care for studying in this paper.
2. LITERATURE REVIEW
The Affordable Care Act is a law which is launched for improving health insurance and expanding insurance coverage to uninsured people. Since the advent of the ACA, it has had a great impact in the U.S. medical system. Because of the ACA, the uninsured people reduced from 16% in 2010 to 9.1% in 2015 (Obama, 2016![]() ). Many studies concern about the effect of the ACA and the use of preventive care. Lau et al. (2014
). Many studies concern about the effect of the ACA and the use of preventive care. Lau et al. (2014![]() ) found that the ACA provision to expand or increase insurance coverage for young adults, and these young adults increase demand for preventive care. Cantor et al. (2012
) found that the ACA provision to expand or increase insurance coverage for young adults, and these young adults increase demand for preventive care. Cantor et al. (2012![]() ) investigated how the ACA affected preventive care among young adults. However, the data they used was from the Current Population Survey 2005-2011, and the data after the ACA is just one year data, it was not large enough.
) investigated how the ACA affected preventive care among young adults. However, the data they used was from the Current Population Survey 2005-2011, and the data after the ACA is just one year data, it was not large enough.
The paper mainly focuses on preventive care, because the primary preventive care is to reduce the occurrence or incidence of disease, and vaccination is one of the primary preventive care. The flu shot is a sort of preventive care. As we know, annual immunization with influenza vaccine is to reduce the effect of infections and can control or reduce diseases. The other preventive care is to do HIV test which is a routine preventive care. In the model regression, I choose flu shot and HIV test as dependent variables to represent preventive care for adults, and preventive cares that I consider in this paper are flu shot and HIV test, there are some academic literatures which also use flu shot and HIV test as preventive care for adults. Lau et al. (2014![]() ) chose flu shot as one of preventive care in their research, and Simon et al. (2017
) chose flu shot as one of preventive care in their research, and Simon et al. (2017![]() ) also chose flu shot and HIV test as preventive care in their research paper. In order to examine my research question, I refer to four papers which introduce how to build model and choose independent variables. Cantor et al. (2012
) also chose flu shot and HIV test as preventive care in their research paper. In order to examine my research question, I refer to four papers which introduce how to build model and choose independent variables. Cantor et al. (2012![]() ) examined the effect of the ACA on health insurance among young adults, and they included demographic variables such as age, gender and race, because these demographic variables are probably associated with the use of preventive care. Hsieh and Lin (1997
) examined the effect of the ACA on health insurance among young adults, and they included demographic variables such as age, gender and race, because these demographic variables are probably associated with the use of preventive care. Hsieh and Lin (1997![]() ) investigated the relationship between health information and demand for preventive care among the elderly, and they showed well-educated people knew health information well, so education potentially affected the demand for preventive care. Also, Hsieh and Lin (1997
) investigated the relationship between health information and demand for preventive care among the elderly, and they showed well-educated people knew health information well, so education potentially affected the demand for preventive care. Also, Hsieh and Lin (1997![]() ) examined that the demographic variables, such as age and gender, could influence on preventive care, and they did find age is positively associated with using preventive care. Kenkel (1990; 1994
) examined that the demographic variables, such as age and gender, could influence on preventive care, and they did find age is positively associated with using preventive care. Kenkel (1990; 1994![]() ) discussed in the relationship between demographic variables (age, gender, race, married status) and preventive care, and he found that demographic variable, such as age, is related to the demand for preventive care. Hsieh and Lin (1997
) discussed in the relationship between demographic variables (age, gender, race, married status) and preventive care, and he found that demographic variable, such as age, is related to the demand for preventive care. Hsieh and Lin (1997![]() ) also discussed that married status could be potentially related to preventive care, and health status could have influence on preventive in their research model. On the basis of these academic literatures, my equation also contains these independent variables, which are age, gender, race, married status, health status and education.
) also discussed that married status could be potentially related to preventive care, and health status could have influence on preventive in their research model. On the basis of these academic literatures, my equation also contains these independent variables, which are age, gender, race, married status, health status and education.
3. DATA
The data source is from the National Health Interview Survey (NHIS), which provides the health information of each individual. The data includes years from 2005 to 2015. All individuals in the data are selected from 18 to 25 years old and 27 to 34 years old. Individuals whose age are 26 years old are excluded from the data, because the NHIS does not mention whether 26 years old is the age-eligibility. In my paper, young adults are considered as 18 – 25 years old who are covered by their parents’ health insurance. I choose the slightly older adults as 27 – 34 years old who cannot be covered by their parents’ health insurance, and the characteristics of slight older adults are similar to the characteristics of young adults. I investigate how the ACA affects preventive care among young adults, so the dependent variables are preventive cares, which are flu shot (Had flu shot vaccine, past 12 months) and HIV Test (Ever tested for HIV) in this study. The independent variables are education; health status and demographic variables, such as gender, race, marital status. Although flu shot and HIV Test are preventive cares, the flu shot is different from HIV Test, so I divide flu shot and HIV Test into two different datasets, but these two datasets include the same independent variables.
Table-1. Population characteristics on flu shot dataset.
Young adults |
Slightly older adults |
|||
| Characteristics | Mean |
Std. |
Mean |
Std. |
| Age | 22.8 |
2.066 |
30.5 |
2.2715 |
| Female | 54.07% |
0.4983 |
52.67% |
0.4993 |
| Education | ||||
| *High school | ||||
| Undergraduate | 48.17% |
0.4997 |
50.23% |
0.5 |
| Master | 5.15% |
0.2211 |
20.29% |
0.4022 |
| Doctor | 0.17% |
0.0418 |
2.69% |
0.1619 |
| Health_status | ||||
| *Excellent | ||||
| Very good | 36.22% |
0.4807 |
37.43% |
0.484 |
| Good | 15.53% |
0.3622 |
16.30% |
0.3694 |
| Fair | 2.31% |
0.1504 |
2.60% |
0.1593 |
| Poor | 0.10% |
0.0319 |
0.20% |
0.0462 |
| Race | ||||
| *White | ||||
| Black | 13% |
0.3404 |
13.07% |
0.3371 |
| Asian | 7.61% |
0.2651 |
10.26% |
0.3035 |
| Married | 16.39% |
0.3702 |
49.32% |
0.5 |
| Observation | 6848 |
14478 |
||
* represents the omitted reference group.
Table-2. Population characteristics on HIV Test dataset.
Young adults |
Slightly older adults |
|||
| Characteristics | Mean |
Std. |
Mean |
Std. |
| Age | 22.8 |
2.063 |
30.5 |
2.2704 |
| Female | 54.09% |
0.4984 |
52.76% |
0.4993 |
| Education | ||||
| *High school | ||||
| Undergraduate | 48.20% |
0.4997 |
50.26% |
0.5 |
| Master | 5.17% |
0.2213 |
20.25% |
0.4018 |
| Doctor | 0.18% |
0.0421 |
2.69% |
0.1617 |
| Health_status | ||||
| *Excellent | ||||
| Very good | 36.14% |
0.4804 |
37.42% |
0.484 |
| Good | 15.50% |
0.3619 |
16.34% |
0.3698 |
| Fair | 2.30% |
0.15 |
2.62% |
0.16 |
| Poor | 0.10% |
0.03213 |
0.22% |
0.0465 |
| Race | ||||
| *White | ||||
| Black | 13.41% |
0.3408 |
13.14% |
0.3378 |
| Asian | 7.61% |
0.2652 |
10.23% |
0.303 |
| Married | 16.42% |
0.3704 |
49.26% |
0.5 |
| Observation | 6754 |
14263 |
||
* represents the omitted reference group.
In Table 1, it shows the mean and the standard deviation of independent variables among young adults and slight older adults who had flu shot in past 12 months. Similarly, Table 2 shows the mean and the standard deviation of independent variables among young adults who ever tested for HIV. The dataset of flu shot includes 17324 individuals, and the dataset of HIV Test includes 17086 individuals.
4. EMPIRICAL STRATEGY
The paper focuses on the provision for young adults in the ACA, and the provision is about expanding health insurance coverage for young adults whose age is under 26 years old, so it would affect the demand for preventive care among young adults. To examine the research question, the simple way is to compare the percentage of utilization of preventive care among young adults between pre the ACA and post the ACA. However, there are no the common trends after the ACA in Figure 1 and Figure 2, and it could be affected by the ACA. On the basis of my research question, I choose Linear Probability Model (LPM) within a D-i-D as my main method. The model equation is:
Lit = α1 + α2 Postt + α3 Age18_25 +α4 Postt * Age18_25 +x’itβ +εit (1)
Where i represents individual, t represents year;
In this equation, Lit are dependent variables which represent flu shot (Had flu shot vaccine, past 12 months) and HIV Test (Ever tested for HIV), and I use Equation 1 to examine whether the effect of the ACA on taking flu shot among young adults and to examine whether the ACA affects using HIV test among young adults.
Postt represents ‘after the ACA’, which means that individual is in the year from 2011 to 2015; Age18_25 represents young adults whose age are from 18 to 25 years old, and it is also the treatment age group in the D-i-D model; Postt * Age18_25 represents the interaction term in D-i-D model, and it means how the ACA has influence on preventive care among young adults; x’it is 1 x 5 row of matrix for individual characteristics which include education, health status, and demographic variables such as gender, race, marital status; εi represents the error term in the equation model.
The Table 3 describes the different situations in Equation 1:
Table-3. The different situations in the model Equation 1.
Before the ACA (2005~2009) |
After the ACA (2011~2015) |
|
Treatment group (18~25 years old) |
α1 + α3 |
α1 + α2 + α3 + α4 |
Control group (27~34 years old) |
α1 |
α1 + α2 |
Source: The Equation 1.
5. RESULTS & DISCUSSION
5.1. Flu Shot
The result is estimated from the effect of the ACA on flu shot among young adults in Table 4. In D-i-D model, I concern about the coefficient of Postt * Age18_25. The coefficient of the interaction term (Postt * Age18_25) on flu shot is 0.159, and its t-value is 1.18, which is not statistically significant, the result suggests that the ACA positively affects the utilization of flu shot among young adults. Since the coefficient of the interaction term on flu shot is statistically insignificant, maybe the ACA does not strongly affect the utilization of flu shot among young adults.
Apparently, the ACA is not the main reason for young adults to increase the use of flu shot, but the Figure 1 shows that the use of flu shot increases year by year. According to the result, one possible explanation is that the flu shot is a sort of common preventive care, which is not expensive, and it is necessary for young adults to take flu shot to keep healthy, in other words, even if young adults are not covered under their parents’ health insurance plan, they still use the flu shot to protect their health from the flu. It seems like that young adults gradually raise their awareness to take flu shot to protect their health.
In the Table 5, there are the results from the effect of other independent variables on flu shot. Since the coefficients of these independent variables reflect how they affect the using of preventive care among adults, it is necessary to analyze the coefficients of these independent variables. The coefficients of Undergraduate, Master degree and Doctor degree are statistically significant, and all the coefficients are positively related to flu shot. According to the coefficients of different degree level, it suggests that adults who receive more education prefer to take flu shot. As we know, if adults receive more education, maybe they have more opportunity to get health information, so that they take flu shot to eliminate or reduce diseases, and this finding is consistent with some studies related to preventive care (Kenkel, 1990; Hsieh and Lin, 1997![]() ). The coefficients of each health status are reasonable, except for ‘Very Good’ health status, the other health statuses such as ‘Good’ ‘Fair’ and ‘Poor’ are statistically significant.
). The coefficients of each health status are reasonable, except for ‘Very Good’ health status, the other health statuses such as ‘Good’ ‘Fair’ and ‘Poor’ are statistically significant.
According to the coefficients of health statuses, it suggests that that adults who report health status as poor tend to use more preventive care, and the result is in line with common sense and is consistent with the finding in the studies related to preventive care (Hsieh and Lin, 1997![]() ) when they are not feel well, they probably prefer to use preventive care to keep healthy. The coefficient of female is statistically significant, and it is 0.0769. Compared to male, females have a lower probability to use flu shot. The coefficient of Married individual is positive and statistically significant, and the coefficient is 0.0551. That is, compared to unmarried adults, married adults are less likely to take flu shot, and the result is close to the finding in Hsieh and Lin (1997
) when they are not feel well, they probably prefer to use preventive care to keep healthy. The coefficient of female is statistically significant, and it is 0.0769. Compared to male, females have a lower probability to use flu shot. The coefficient of Married individual is positive and statistically significant, and the coefficient is 0.0551. That is, compared to unmarried adults, married adults are less likely to take flu shot, and the result is close to the finding in Hsieh and Lin (1997![]() ). Except for Asian people in U.S., the coefficients of other race are statistically significant. Compare to the White people, the coefficient of black people is less like to take flu shot.
). Except for Asian people in U.S., the coefficients of other race are statistically significant. Compare to the White people, the coefficient of black people is less like to take flu shot.
5.2. HIV Test
I also choose the D-i-D model to examine how the ACA affects HIV Test among young adults. In D-i-D model, I concern about the interaction term on HIV Test. In the Table 4 the coefficient of interaction term is -0.00544, and its t-value is -0.35. The coefficient of interaction term on HIV Test is negative, which means that the ACA negatively affects the using of HIV Test among young adults, however, its t-value is less than 1.96 and greater than -1.96, so the coefficient of interaction term on HIV Test is statistically insignificant. According to the result, maybe the ACA does not strongly affect HIV Test among young adults.
In Figure 2, it shows that the percentage of using HIV Test among young adults decreases after 2010. On the basis of the situation, one possible explanation on this finding is that these adults know how to keep their sex life healthy, or they know what the safe sex is, and young adults gradually raise healthy awareness, so that they use less HIV Test. The other possible reason is that these adults lack of knowledge about HIV, and they decrease awareness in doing HIV Test. As a matter of fact, there is no evidence to figure out the certain reasons, and this argument requires a further research.
Table-4. The main results from D-i-D model.
Preventive care |
|||
Variables |
Flu shot |
HIV test |
|
1.Age18_25 |
-0.0161 |
-0.168*** |
|
(-1.54) |
(-15.13) |
||
1.Post_theACA |
-0.150*** |
0.0383*** |
|
(-18.82) |
(4.23) |
||
1.Age18_25*Post |
0.0159 |
-0.00544 |
|
(1.18) |
(-0.35) |
||
T- values in parentheses.
*** p<0.01, ** p<0.05, * p<0.1.
In the Table 5, there are some other independent variables included in this equation model. The coefficients of all degree levels are statistically insignificant, which means that education is not related to the utilization of HIV Test. The coefficients of all health statuses are reasonable, except for ‘Very Good’ health status, the other three health statuses (‘Good’ ‘Fair’ and ‘Poor’) are statistically significant.
According to the coefficients of health statuses, it suggests that adults who report health status as poor tend to do more HIV Test, and this result is in line with common sense, when adults feel unhealthy, they tend to take preventive cares. In term of gender, the coefficient of female is 0.143, which is positive and statistically significant. Compared to male, female is less likely to check for HIV. The coefficient of Married individual status is statistically insignificant, and it implied that married status is not related to do HIV Test. One possible reason is that married adults have stable relationship with their partners, and they have the safe sex, so it is not necessary for them to use HIV Test. The coefficient of each race is statistically significant. Comparing to the Whites, the blacks tend to take more HIV Test, and the Asians tend to take less HIV Test.
Table-5. The whole results from linear probability model within D-i-D.
Preventive care |
|||
Variables |
Flu shot |
HIV test |
|
1.Undergraduate |
0.0829*** |
0.00873 |
|
(0.00718) |
(0.00845) |
||
2.Master degree |
0.115*** |
0.00761 |
|
(0.0109) |
(0.0120) |
||
3.Doctoral degree |
0.194*** |
0.00505 |
|
(0.0277) |
(0.0286) |
||
1.Very Good |
-0.00556 |
0.000601 |
|
(0.00722) |
(0.00818) |
||
2.Good |
0.0169* |
0.0324*** |
|
(0.00962) |
(0.0108) |
||
3.Fair |
0.0601*** |
0.0656*** |
|
(0.0221) |
(0.0233) |
||
4.Poor |
0.175** |
0.268*** |
|
(0.0832) |
(0.0706) |
||
1.Female |
0.0769*** |
0.143*** |
|
(0.00654) |
(0.00742) |
||
1.Married |
0.0551*** |
0.000163 |
|
(0.00717) |
(0.00810) |
||
1.Black |
-0.0203** |
0.249*** |
|
(0.00950) |
(0.0103) |
||
2.Asian |
0.0128 |
-0.0545*** |
|
(0.0124) |
(0.0133) |
||
1.Age18_25 |
-0.0161 |
-0.168*** |
|
(0.0105) |
(0.0111) |
||
1.Post_theACA |
-0.150*** |
0.0383*** |
|
(0.00797) |
(0.00905) |
||
1.Age18_25*Post |
0.0159 |
-0.00544 |
|
(0.0135) |
(0.0156) |
||
Constant |
0.207*** |
0.408*** |
|
(0.00980) |
(0.0114) |
||
Observations |
17,324 |
17,086 |
|
R-squared |
0.057 |
0.085 |
|
Robust standard errors in parentheses.
*** p<0.01, ** p<0.05, * p<0.1.
6. CONCLUSION
In this paper, I focus on the ACA and preventive care among young adults, and I put forward a research question is whether the ACA affects preventive care among young adults. As we know, the Affordable Care Act is a policy, which was passed by 2010. The main goal of the ACA is to reduce the number of uninsured people and make health service affordable, and the ACA expands Medicaid eligibility and health insurance coverage.
If Medicaid eligibility and health insurance coverage are expanded, or health insurance can cover some parts of cost of preventive care, so people who benefit from the ACA tend to preventive cares. There are many provisions in the ACA, but I just focus on one provision for young adults, and this provision is that dependents whose age is up to 26 years old can be covered by their parents’ health insurance plan. Perhaps, the ACA can affect preventive care among young adults. In order to investigate this research question, I pick up the data from National Health Interview Survey (NHIS) and design my model as Linear Probability Model within a difference in difference. In D-i-D, I choose young adults whose age are 18- 25 years old as the treatment group and slightly old adults as the control group, comparing the utilization of preventive care between these two age groups pre the ACA and post the ACA.
Finally, I examine two preventive cares for studying in this paper, these two preventive cares are flu shot and HIV Test. In the results, the coefficient of the interaction term on flu shot is statistically insignificant, which means that the ACA does not strongly affect utilization of flu shot among young adults. When young adults choose flu shot, they do not care about whether they are covered by their parents’ health insurance plan, but the Figure 1 shows that the percentage of taking flu shot among young adults increase year by year.
Perhaps, the flu shot is a common preventive care and not expensive, so young adults would like to use the flu shot to protect them from the flu, in some sense, the finding shows that young adults gradually raise awareness to take flu shot to protect their health from the flu. Also, the coefficient of the interaction term on HIV Test is statistically insignificant, which means that the ACA does not strongly affect utilization of HIV Test among young adults. However, after the ACA, the using of HIV Test decreases year by year, and checking HIV is not ‘popular’. One possible explanation is that HIV Test is not a common preventive care, which is just for adults who really need to take HIV Test.
| Funding: This study received no specific financial support. |
| Competing Interests: The author declares that there are no conflicts of interests regarding the publication of this paper. |
REFERENCES
Ai, C. and E.C. Norton, 2003. Interaction terms in logit and probit models. Economics Letters, 80(1): 123-129.Available at: https://doi.org/10.1016/s0165-1765(03)00032-6.
Cantor, J.C., A.C. Monheit, D. DeLia and K. Lloyd, 2012. Early impact of the affordable care act on health insurance coverage of young adults. Health Services Research, 47(5): 1773-1790.Available at: https://doi.org/10.1111/j.1475-6773.2012.01458.x.
Carman, K.G., C. Eibner and S.M. Paddock, 2015. Trends in health insurance enrollment, 2013–15. Health Affairs, 34(6): 1044-1048.Available at: https://doi.org/10.1377/hlthaff.2015.0266.
Coffin, J. and S. Rak, 2013. Affordable care act. The Journal of Medical Practice Manage, 28(5): 317-319.
Faulkner, L.A. and H.H. Schauffler, 1997. The effect of health insurance coverage on the appropriate use of recommended clinical preventive services. American Journal of Preventive Medicine, 13(6): 453-458.Available at: https://doi.org/10.1016/s0749-3797(18)30141-7.
Finkelstein, A., S. Taubman, B. Wright, M. Bernstein, J. Gruber, J.P. Newhouse, H. Allen, K. Baicker and O.H.S. Group, 2012. The Oregon health insurance experiment: Evidence from the first year. The Quarterly Journal of Economics, 127(3): 1057-1106.Available at: https://doi.org/10.1093/qje/qjs020.
Hsieh, C.-R. and S.-J. Lin, 1997. Health information and the demand for preventive care among the elderly in Taiwan. Journal of Human Resources, 32(2): 308-333.Available at: https://doi.org/10.2307/146217.
Institute of Medicine (U. S.), 2010. Priorities for the national vaccine plan. National Academies Press.
Kenkel, D., 1990. Consumer health information and the demand for medical care. The Review of Economics and Statistics, 72(4): 587-595.Available at: https://doi.org/10.2307/2109598.
Kenkel, D.S., 1990; 1994. The demand for preventive medical care. Applied Economics, 26(4): 313-325.Available at: https://doi.org/10.1080/00036849400000078.
Lau, J.S., S.H. Adams, W.J. Boscardin and C.E. Irwin Jr, 2014. Young adults' health care utilization and expenditures prior to the affordable care act. Journal of Adolescent Health, 54(6): 663-671.Available at: https://doi.org/10.1016/j.jadohealth.2014.03.001.
Lau, J.S., S.H. Adams, M.J. Park, W.J. Boscardin and C.E. Irwin, 2014. Improvement in preventive care of young adults after the affordable care act: The affordable care act is helping. JAMA Pediatrics, 168(12): 1101-1106.Available at: https://doi.org/10.1001/jamapediatrics.2014.1691.
Obama, B., 2016. United States health care reform: Progress to date and next steps. Jama, 316(5): 525-532.Available at: https://doi.org/10.1001/jama.2016.9797.
Simon, K., A. Soni and J. Cawley, 2017. The impact of health insurance on preventive care and health behaviors: Evidence from the first two years of the ACA Medicaid expansions. Journal of Policy Analysis and Management, 36(2): 390-417.Available at: https://doi.org/10.1002/pam.21972.
Views and opinions expressed in this article are the views and opinions of the author(s), International Journal of Asian Social Science shall not be responsible or answerable for any loss, damage or liability etc. caused in relation to/arising out of the use of the content. |