




THE KNOWLEDGE, PERCEPTIONS, ATTITUDES, AND PERCEIVED RISK IN HIV/AIDS AMONG WOMEN IN MALAYSIA: A CROSS-SECTIONAL STUDY

1Senior Lecturer, Department of Communication, Faculty of Modern Languages and Communication, Universiti Putra Malaysia, Serdang, Malaysia
ABSTRACT
The remarkable challenge in alleviating HIV/AIDS rates in Malaysia continued from its first case in 1986. Since then, a number of government initiatives have been put in place to address the escalating rates of HIV/AIDS especially among people who inject the drug (PWID). While HIV infections among intravenous drug users reportedly saw a steady decline, we seem to be leaving some people behind—women. This study seeks to examine HIV/AIDS knowledge, perceptions, attitudes, and perceived risk among women in Malaysia. We recruited 384 respondents, including 170 males and 210 females. As this research focused on women, 210 females were therefore selected for data analysis. The results show that the knowledge of HIV/AIDS modes of transmission among the surveyed respondents were rather high. However, there were some respondents who still believed that kissing and sharing utensils are the modes of HIV/AIDS transmission. Most of the respondents had moderate positive perceptions and a discriminatory attitude towards people living with HIV/AIDS (PLHIV). In terms of respondents' perception of risk of HIV/AIDS infection, surveyed respondents did not perceive themselves to be at risk of HIV infection. Nevertheless, they would protect themselves or their partners from HIV/AIDS infection by using condoms. More open discussion about HIV/AIDS should be held not only to raise the level of awareness but also to promote healthier behaviour and eliminate stigma and discrimination towards PLHIV.
Keywords:HIV/AIDS Women Knowledge perception Perceived risk Malaysia.
ARTICLE HISTORY: Received:12 June 2018. Revised:12 July 2018. Accepted:16 July 2018. Published:20 July 2018.
Contribution/ Originality:This study contributes in the existing literature on women’s knowledge, perceptions, attitudes and perceived risk of HIV/AIDS and people living with HIV/AIDS. The paper’s primary contribution is finding that surveyed women do not think that they are at risk of HIV/AIDS infection.
1. INTRODUCTION
HIV/AIDS in Malaysia was, initially, dominated by people who inject the drug (PWID) and therefore, we are classified by the World Health Organization (WHO) as a “concentrated epidemic” country (AIDS/STD Section, 2010 ![]() ). Since then, the Malaysian government remains unswerving in the commitment to halting and responding to the epidemic. Various government responses and initiatives have been put in place to tackle the epidemic efficaciously in the country. From pre-marital HIV Testing, Harm Reduction Programme and to the recent National Strategic Plan for Ending AIDS 2016-2030 in responding to ending HIV/AIDS in Malaysia, the new HIV infection has declined by half, falling from 22 per 100,000 populations in 2000 to 10.9 per 100,000 populations in 2015 (HIV/STI Section, 2015
). Since then, the Malaysian government remains unswerving in the commitment to halting and responding to the epidemic. Various government responses and initiatives have been put in place to tackle the epidemic efficaciously in the country. From pre-marital HIV Testing, Harm Reduction Programme and to the recent National Strategic Plan for Ending AIDS 2016-2030 in responding to ending HIV/AIDS in Malaysia, the new HIV infection has declined by half, falling from 22 per 100,000 populations in 2000 to 10.9 per 100,000 populations in 2015 (HIV/STI Section, 2015 ![]() ). The number of HIV/AIDS-related deaths also stabilised during the same period. Notwithstanding the government has made impressive efforts at achieving results and reaching out PWID to reverse this epidemic, we seem to be leaving some people behind—women. AIDS was first spread among homosexual groups, injecting drug users and commercial female sex workers from the United States and in most of the other countries (Centers for Disease Control and Prevention (CDC), 2001
). The number of HIV/AIDS-related deaths also stabilised during the same period. Notwithstanding the government has made impressive efforts at achieving results and reaching out PWID to reverse this epidemic, we seem to be leaving some people behind—women. AIDS was first spread among homosexual groups, injecting drug users and commercial female sex workers from the United States and in most of the other countries (Centers for Disease Control and Prevention (CDC), 2001 ![]() ; U.S. Department of Health and Human Services, 2001
; U.S. Department of Health and Human Services, 2001 ![]() ; Singhal and Rogers, 2003
; Singhal and Rogers, 2003 ![]() ). In Malaysia, HIV infection was common among intravenous drug users or to be exact, people who inject the drug (PWID). These people contributed 70-80 percent of all newly reported cases. Yet, the trend has presently changed. This group spreads further to sexual partners of whom they are innocent wives and commercial female sex workers (United Nations Children’s Fund, 2008
). In Malaysia, HIV infection was common among intravenous drug users or to be exact, people who inject the drug (PWID). These people contributed 70-80 percent of all newly reported cases. Yet, the trend has presently changed. This group spreads further to sexual partners of whom they are innocent wives and commercial female sex workers (United Nations Children’s Fund, 2008 ![]() ; Mondal and Shitan, 2013
; Mondal and Shitan, 2013 ![]() ; HIV/STI Section, 2015
; HIV/STI Section, 2015 ![]() ). Globally, 18.6 million girls and women were living with HIV in 2015, and nearly one million girls and women were newly infected with HIV in the same year (Joint United Nations Programme on HIV/AIDS, 2017
). Globally, 18.6 million girls and women were living with HIV in 2015, and nearly one million girls and women were newly infected with HIV in the same year (Joint United Nations Programme on HIV/AIDS, 2017 ![]() ). In Malaysia, as of December 2015, about 12,165 women and girls in Malaysia have acquired HIV since 1986 (HIV/STI Section, 2015
). In Malaysia, as of December 2015, about 12,165 women and girls in Malaysia have acquired HIV since 1986 (HIV/STI Section, 2015 ![]() ).
).
The Malaysian Ministry of Health (MOH) recorded a total of 3,300 new HIV infections with 512 newly reported HIV cases were women in 2015 (HIV/STI Section, 2015 ![]() ). The profile of female HIV cases in 2014 indicated that close to 20 percent were young (<25 years old), about half (45%) were Malays, 92% had acquired HIV through heterosexual transmission and 40 percent were housewives (HIV/STI Section, 2015
). The profile of female HIV cases in 2014 indicated that close to 20 percent were young (<25 years old), about half (45%) were Malays, 92% had acquired HIV through heterosexual transmission and 40 percent were housewives (HIV/STI Section, 2015 ![]() ). According to the Malaysian Ministry of Health, housewives being infected with HIV is worrisome and they are five times at risk of than female sex workers (UNICEF, 2008
). According to the Malaysian Ministry of Health, housewives being infected with HIV is worrisome and they are five times at risk of than female sex workers (UNICEF, 2008 ![]() ; Najimudeen and Rosy, 2011
; Najimudeen and Rosy, 2011 ![]() ; Munusamy and Fadzil, 2017
; Munusamy and Fadzil, 2017 ![]() ). When the United States received its first HIV/AIDS case, many national policies and the Centers for Disease Control and Prevention (CDC) failed to address and recognize heterosexual transmission (Higgins et al., 2010
). When the United States received its first HIV/AIDS case, many national policies and the Centers for Disease Control and Prevention (CDC) failed to address and recognize heterosexual transmission (Higgins et al., 2010 ![]() ). Women, therefore, were absent from clinical trials (Fox-Tierney et al., 1999
). Women, therefore, were absent from clinical trials (Fox-Tierney et al., 1999 ![]() ). Likewise, this scenario can be seen in Malaysia, where much attention was given to injecting drug users at the beginning of the epidemic as they were the main driver of HIV/AIDS infection in the country since 1986. Thus, women were nearly invisible at that point in time with regard to public health aid. Only in recent years, the increasingly feminised nature of the HIV epidemic in the country has received intensive attention from various stakeholders. The Malaysian government, especially, realises the significance of addressing the issue and is committed to tackling the issue by outlining its fourth strategy of reducing HIV vulnerability among women, young people and children in the National Strategic Plan on HIV/AIDS 2006-2010 (NSP). The government is of the view that women and girls play a vital role in the family and community as mothers and caregivers. When they are infected with HIV, they can pass the virus on to their future children at birth or through breastfeeding as well as those who will be prematurely orphaned. The under-representation of women in HIV/AIDS research leads to gaps in the scientific knowledge about why women are vulnerable to HIV/AIDS. Little is known about how much knowledge Malaysian women have of HIV/AIDS and their perceptions and attitudes towards HIV/AIDS. This information is overarching for developing much-needed conversations on improving sexual and reproductive health awareness amongst women in Malaysia. By doing so, targeted and effective education programmes about HIV/AIDS can be suggested. This paper begins by explaining the reasons of women are so vulnerable to HIV/AIDS from both scientific and social perspectives. The author also reviews past studies on women's level of knowledge, perceptions and perceived risk of HIV/AIDS. After reviewing relevant literature, this is followed by how the data is collected and what the study reveals as well as how it can extend our current understanding of women's perceptions, attitudes and perceived risk of HIV/AIDS in Malaysia context.
). Likewise, this scenario can be seen in Malaysia, where much attention was given to injecting drug users at the beginning of the epidemic as they were the main driver of HIV/AIDS infection in the country since 1986. Thus, women were nearly invisible at that point in time with regard to public health aid. Only in recent years, the increasingly feminised nature of the HIV epidemic in the country has received intensive attention from various stakeholders. The Malaysian government, especially, realises the significance of addressing the issue and is committed to tackling the issue by outlining its fourth strategy of reducing HIV vulnerability among women, young people and children in the National Strategic Plan on HIV/AIDS 2006-2010 (NSP). The government is of the view that women and girls play a vital role in the family and community as mothers and caregivers. When they are infected with HIV, they can pass the virus on to their future children at birth or through breastfeeding as well as those who will be prematurely orphaned. The under-representation of women in HIV/AIDS research leads to gaps in the scientific knowledge about why women are vulnerable to HIV/AIDS. Little is known about how much knowledge Malaysian women have of HIV/AIDS and their perceptions and attitudes towards HIV/AIDS. This information is overarching for developing much-needed conversations on improving sexual and reproductive health awareness amongst women in Malaysia. By doing so, targeted and effective education programmes about HIV/AIDS can be suggested. This paper begins by explaining the reasons of women are so vulnerable to HIV/AIDS from both scientific and social perspectives. The author also reviews past studies on women's level of knowledge, perceptions and perceived risk of HIV/AIDS. After reviewing relevant literature, this is followed by how the data is collected and what the study reveals as well as how it can extend our current understanding of women's perceptions, attitudes and perceived risk of HIV/AIDS in Malaysia context.
2. LITERATURE REVIEW
2.1. Women and HIV/AIDS – Susceptibility, Vulnerability and Beyond
The feminisation of the HIV epidemic in this region is rapidly occurring in Malaysia. On that count, it is more than just an issue of preventing or/and controlling the spread of the disease, but it is also pertinent to develop understanding and respond to the vulnerabilities and risks related to gender discrimination and inequality, cultural and religious norms, expectations and economics. Therefore, understanding why women are vulnerable to HIV/AIDS and STD infection is utmost critical and necessary for developing and implementing effective prevention programme. Women are always labeled as a vulnerable group to HIV/AIDS infection due to their biological susceptibility, reduced sexual autonomy and men’s sexual power and privilege (Women’s Aid Organisation, 2001 ![]() ; Higgins et al., 2010
; Higgins et al., 2010 ![]() ; Mondal and Shitan, 2013
; Mondal and Shitan, 2013 ![]() ; Wagbara, 2017
; Wagbara, 2017 ![]() ). This proposition is explained in a model termed “vulnerability paradigm”—a model that explains the aetiology and evolution of women become the primary vulnerable victims of HIV epidemic. The major pillar of the paradigm describes gender-based social inequalities in which women are lacking the power to protect themselves from contracting HIV/AIDS, and men are more likely than women to affect their partners because they engage in more sexual and drug use risk behaviours. In other words, men are active transmitters of HIV but not active agents of prevention (Higgins et al., 2010
). This proposition is explained in a model termed “vulnerability paradigm”—a model that explains the aetiology and evolution of women become the primary vulnerable victims of HIV epidemic. The major pillar of the paradigm describes gender-based social inequalities in which women are lacking the power to protect themselves from contracting HIV/AIDS, and men are more likely than women to affect their partners because they engage in more sexual and drug use risk behaviours. In other words, men are active transmitters of HIV but not active agents of prevention (Higgins et al., 2010 ![]() ). Literature also showed that women have upward of twice the probability of infection if they exposed to HIV (Padian et al., 1991
). Literature also showed that women have upward of twice the probability of infection if they exposed to HIV (Padian et al., 1991 ![]() ; Nicolosi et al., 1994
; Nicolosi et al., 1994 ![]() ; Royce et al., 1997
; Royce et al., 1997 ![]() ; Mastro and Kitayaporn, 1998
; Mastro and Kitayaporn, 1998 ![]() ; UNICEF, 2008
; UNICEF, 2008 ![]() ). Research explicated that biologically, women are more vulnerable to HIV/AIDS infection through vaginal intercourse in that they are exposed to infectious fluids for long periods of time during sexual intercourse than men are (Bolan et al., 1999
). Research explicated that biologically, women are more vulnerable to HIV/AIDS infection through vaginal intercourse in that they are exposed to infectious fluids for long periods of time during sexual intercourse than men are (Bolan et al., 1999 ![]() ). During sexual intercourse, the vagina faces increased risk of tissue injury, and this allows the vagina for a greater possibility of entry of the virus (Bolan et al., 1999
). During sexual intercourse, the vagina faces increased risk of tissue injury, and this allows the vagina for a greater possibility of entry of the virus (Bolan et al., 1999 ![]() ; Huang, 2002
; Huang, 2002 ![]() ). Younger girls are especially vulnerable because their immature mucosal surfaces are even more easily torn during sexual intercourse (Huang, 2002
). Younger girls are especially vulnerable because their immature mucosal surfaces are even more easily torn during sexual intercourse (Huang, 2002 ![]() ).
).
HIV/AIDS infection among women is also clearly portrayed not only through biological susceptibility, but also socio-economic differences and cultural conservative. Mane and Maitra (1992 ![]() ) revealed that in countries such as India, women’s powerlessness is glorified in a pativrata (dedication to the husband) image, which portrays women as loyal and subordinate to their husbands, even when neglected, ill-treated, or deserted (as cited in (Singhal and Rogers, 2003
) revealed that in countries such as India, women’s powerlessness is glorified in a pativrata (dedication to the husband) image, which portrays women as loyal and subordinate to their husbands, even when neglected, ill-treated, or deserted (as cited in (Singhal and Rogers, 2003 ![]() )). The pativrata women, unfortunately, dutifully engage in unprotected sex with her husband, despite knowing her partner's HIV-positive status (Singhal and Rogers, 2003
)). The pativrata women, unfortunately, dutifully engage in unprotected sex with her husband, despite knowing her partner's HIV-positive status (Singhal and Rogers, 2003 ![]() ). Past research revealed that Black and Latina's women were most likely to contract HIV heterosexually as they lived in the poorest sections of the US cities that were hit by the deindustrialisation of the 1970s (Zierler and Kriger, 1997
). Past research revealed that Black and Latina's women were most likely to contract HIV heterosexually as they lived in the poorest sections of the US cities that were hit by the deindustrialisation of the 1970s (Zierler and Kriger, 1997 ![]() ; Dworkin, 2005
; Dworkin, 2005 ![]() ). These women mostly contracted the virus from men who were injecting drug users or had intercourse with men or other women, including female sex workers (Guinan and Hardy, 1987
). These women mostly contracted the virus from men who were injecting drug users or had intercourse with men or other women, including female sex workers (Guinan and Hardy, 1987 ![]() ; Wortley and Fleming, 1997; Kamb and Wortley, 2000
; Wortley and Fleming, 1997; Kamb and Wortley, 2000 ![]() ). Likewise, in Nigeria, gender inequality significantly impacts women's knowledge and awareness of the transmission of HIV/AIDS. Traditional beliefs, religion, and polygamy are contributing factors to gender inequality and thereafter to HIV/AIDS infections (Wagbara, 2017
). Likewise, in Nigeria, gender inequality significantly impacts women's knowledge and awareness of the transmission of HIV/AIDS. Traditional beliefs, religion, and polygamy are contributing factors to gender inequality and thereafter to HIV/AIDS infections (Wagbara, 2017 ![]() ). The trend can also be seen in Malaysia context. Copious research showed that the risk factor identified among HIV-infected pregnant and women is sexual intercourse with their partners, and these partners involved in risky behaviours such as injecting drug and sexual activities (Fauziah et al., 2002
). The trend can also be seen in Malaysia context. Copious research showed that the risk factor identified among HIV-infected pregnant and women is sexual intercourse with their partners, and these partners involved in risky behaviours such as injecting drug and sexual activities (Fauziah et al., 2002 ![]() ; Huang, 2002
; Huang, 2002 ![]() ; Allison and Seeley, 2004
; Allison and Seeley, 2004 ![]() ; Kissling et al., 2005
; Kissling et al., 2005 ![]() ; Kelantanese Women top List of those Infected with HIV/Aids, 2010
; Kelantanese Women top List of those Infected with HIV/Aids, 2010 ![]() ; Samsudin et al., 2011
; Samsudin et al., 2011 ![]() ). The overlap between injecting drug use and commercial sex work contributes to the rapid spread of HIV/AIDS. These people are at double risk for infection through both heterosexual intercourse and sharing contaminated needles. Housewives and female partners are, therefore, vulnerable and innocent to contract the virus from their husbands and male partners who are injecting drug users and involve in sexual activity (i.e., seeking commercial sex). Figure 1 illustrates the complex relationship among different groups who are associated with possible HIV/AIDS transmission.
). The overlap between injecting drug use and commercial sex work contributes to the rapid spread of HIV/AIDS. These people are at double risk for infection through both heterosexual intercourse and sharing contaminated needles. Housewives and female partners are, therefore, vulnerable and innocent to contract the virus from their husbands and male partners who are injecting drug users and involve in sexual activity (i.e., seeking commercial sex). Figure 1 illustrates the complex relationship among different groups who are associated with possible HIV/AIDS transmission.
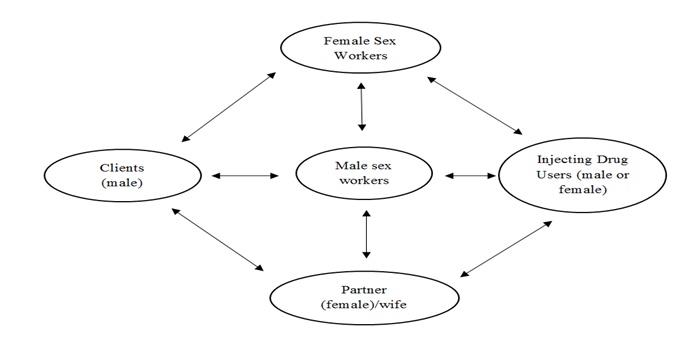
Figure-1. Dynamic relationships among populations at risk. Adapted and modified from UNICEF (2008 ![]() ) p.42.
) p.42.
Source: UNICEF (2008 ![]() ).
).
Economically, sex workers (both male and female) who are also injectors are forced to engage in transactional sex so that they are able to finance their drug use, which indirectly exposes them to the risk of HIV/AIDS infection. Contaminated needles are shared between sex workers and clients who pay sex with drugs. Some clients pay sex with money and engage in unprotected sex (without using condoms or low in using condoms) with sex workers. In these conditions, clients, be they pay sex with drugs or money also engage in unprotected sex with their wives and partners, thereafter pass the infection on to them. Toeing to that thought, housewives and women are vulnerable to the infection. Socially and culturally, the inability to negotiate condom use has become an indicator of HIV/AIDS growth among married women and sex workers. Research showed that women are vulnerable to acquiring HIV due to inability to communicate and negotiate sex with their partners even though they are aware of their partners' seropositive status (UNICEF, 2008![]() ; Wagbara, 2017
; Wagbara, 2017 ![]() ). Sex workers are also unable to negotiate condom use with clients even though condom is deemed to be one of the prophylactic measures suggested and emphasised by most of the public health practitioners all over the world. In the effort of preventing the spread of HIV/AIDS, one should not merely focus on female sex workers who are blamed to be the supply chain of the infection. In fact, addressing and acknowledging the complex dynamics shown in Figure 1 is rather cardinal. When unequal gender relations, unequal power relations and lack negotiating power obstructs any prevention such as condom use, participation among clients and husbands in this context is crucial. When couples are able to communicate their sexual needs and intent, they also may find it easier to communicate about family planning, reproductive intentions, family size and sexual health including HIV/AIDS.
). Sex workers are also unable to negotiate condom use with clients even though condom is deemed to be one of the prophylactic measures suggested and emphasised by most of the public health practitioners all over the world. In the effort of preventing the spread of HIV/AIDS, one should not merely focus on female sex workers who are blamed to be the supply chain of the infection. In fact, addressing and acknowledging the complex dynamics shown in Figure 1 is rather cardinal. When unequal gender relations, unequal power relations and lack negotiating power obstructs any prevention such as condom use, participation among clients and husbands in this context is crucial. When couples are able to communicate their sexual needs and intent, they also may find it easier to communicate about family planning, reproductive intentions, family size and sexual health including HIV/AIDS.
2.2. Women's Knowledge, Perceptions and Perceived Risk of HIV/AIDS
Recent studies in Malaysia (Wan et al., 2012 ![]() ; Mohd Saad et al., 2013
; Mohd Saad et al., 2013 ![]() ; Munusamy and Fadzil, 2017
; Munusamy and Fadzil, 2017 ![]() ), Nigeria and Democratic Republic of Congo (Gebremedhin et al., 2017
), Nigeria and Democratic Republic of Congo (Gebremedhin et al., 2017 ![]() ); India (Hazarika, 2010
); India (Hazarika, 2010 ![]() ); Zambia (Mutombo and Maina, 2015
); Zambia (Mutombo and Maina, 2015 ![]() ) Iran (Tafazoli et al., 2016
) Iran (Tafazoli et al., 2016 ![]() ) and Saudi Arabia (Alwafi et al., 2018
) and Saudi Arabia (Alwafi et al., 2018 ![]() ) have revealed that women (including female sex workers) have generally low knowledge about HIV/AIDS but have positive attitudes towards HIV/AIDS. There are positive associations between levels of HIV/AIDS knowledge, attitudes, HIV risk perception and education level of which the higher a woman's education, the highest her levels of knowledge about, the perception of HIV/AIDS risk (in relation to condom use) and positive acceptance attitudes towards HIV/AIDS. For example, Munusamy and Fadzil (2017
) have revealed that women (including female sex workers) have generally low knowledge about HIV/AIDS but have positive attitudes towards HIV/AIDS. There are positive associations between levels of HIV/AIDS knowledge, attitudes, HIV risk perception and education level of which the higher a woman's education, the highest her levels of knowledge about, the perception of HIV/AIDS risk (in relation to condom use) and positive acceptance attitudes towards HIV/AIDS. For example, Munusamy and Fadzil (2017 ![]() ) reported that Indian Malaysian women lack knowledge and awareness on HIV/AIDS which further lead to many of these women were unaware that HIV can be transmitted through their husbands. In the same year, a Nigerian study found despite high level of awareness of HIV/AIDS among Nigerian and Congolese young women, their level of knowledge on the subject matter was still low, and it is actually far below the target set in 2001 by the United Nations General Assembly Special Session (UNGASS) which aims to ensure 95 per cent of young people aged 15-24 worldwide have access to correct information, services necessary to boost the life skills needed to reduce their risk of HIV infection (Gebremedhin et al., 2017
) reported that Indian Malaysian women lack knowledge and awareness on HIV/AIDS which further lead to many of these women were unaware that HIV can be transmitted through their husbands. In the same year, a Nigerian study found despite high level of awareness of HIV/AIDS among Nigerian and Congolese young women, their level of knowledge on the subject matter was still low, and it is actually far below the target set in 2001 by the United Nations General Assembly Special Session (UNGASS) which aims to ensure 95 per cent of young people aged 15-24 worldwide have access to correct information, services necessary to boost the life skills needed to reduce their risk of HIV infection (Gebremedhin et al., 2017 ![]() ). Gebremedhin and his colleagues also found that the acceptance attitude of young women in both countries towards people living with HIV/AIDS (PLHIV) was also low. They found a significant association between acceptance attitude towards PLHIV among the respondents and their level of education. The similar study also reported in Zambia, where Zambian women had less tolerant towards people living with HIV/AIDS than Zambian men, and the reason was due to the low level of HIV/AIDS knowledge among women as misinformation is a source of stigma (Mutombo and Maina, 2015
). Gebremedhin and his colleagues also found that the acceptance attitude of young women in both countries towards people living with HIV/AIDS (PLHIV) was also low. They found a significant association between acceptance attitude towards PLHIV among the respondents and their level of education. The similar study also reported in Zambia, where Zambian women had less tolerant towards people living with HIV/AIDS than Zambian men, and the reason was due to the low level of HIV/AIDS knowledge among women as misinformation is a source of stigma (Mutombo and Maina, 2015 ![]() ). However, generalising these findings to Malaysian women is teething mainly because Malaysia is more conservative, where religious and cultural taboos in the discussion of sexuality have made the visibility of HIV prevention and treatment programmes largely impossible among the public (Tham and Zanuddin, 2015
). However, generalising these findings to Malaysian women is teething mainly because Malaysia is more conservative, where religious and cultural taboos in the discussion of sexuality have made the visibility of HIV prevention and treatment programmes largely impossible among the public (Tham and Zanuddin, 2015 ![]() ). Toeing to that line, a survey of Malaysian women was therefore required. This article examines HIV/AIDS knowledge, perceptions, attitudes, and perceived risk among women in Malaysia so as to provide base information to policymakers, health public relations practitioners and the media to outline, advocate and promote national policies and communication campaigns that focus more on women in HIV/AIDS prevention in this setting.
). Toeing to that line, a survey of Malaysian women was therefore required. This article examines HIV/AIDS knowledge, perceptions, attitudes, and perceived risk among women in Malaysia so as to provide base information to policymakers, health public relations practitioners and the media to outline, advocate and promote national policies and communication campaigns that focus more on women in HIV/AIDS prevention in this setting.
3. RESEARCH METHOD
A stratified random sampling was implemented in Klang Valley. Based on a list of demographics obtained from the Department of Statistics Malaysia, Klang Valley is categorised into six districts: (1) Federal Territory of Kuala Lumpur, (2) Gombak, (3) Klang, (4) Petaling, (5) Sepang and (6) Ulu Langat. Three hundred and eighty-four respondents, including 174 males and 210 females, were recruited for the study using Krejcie and Morgan’s formula (Krejcie and Morgan, 1970 ![]() ). As this research focused on women, 210 females were therefore selected for data analysis. The survey questionnaire was administered by the author. Prospective survey respondents were screened based on whether or not they had heard of Human Immunodeficiency Virus (HIV) or Acquired Immunodeficiency Syndrome (AIDS). A total of three female respondents had never heard of neither HIV nor AIDS, and were therefore excluded from the study. This study’s findings and analyses of female respondents' knowledge, perceptions, attitudes, and personal perceived risk of HIV/AIDS were, therefore, based on the remaining 207 female respondents. The survey questionnaire included items measuring respondents’ knowledge of HIV/AIDS transmission modes, perceptions and attitudes towards PLHIV and personal perceived risk of HIV/AIDS. There were 10 items to assess female respondents’ knowledge about HIV/AIDS (Cronbach’s Alpha = .83). Twelve items were designed to measure respondents’ perceptions of PLHIV and attitudes towards PLHIV respectively (Cronbach's Alpha = .72 for both). These items were plotted on a 5-point Likert scale; from strongly disagree to strongly agree. Three items, using dichotomous measurement ("agree" or "disagree"), assessed female respondents' personal perceived risk of HIV/AIDS. Data were recorded and analysed using the Statistical Package for the Social Science (SPSS 20.0). Statistical analysis included parametric statistics (i.e., Pearson correlation and T-test) and nonparametric statistics (i.e., frequencies, percentages, mean, and standard deviation).
). As this research focused on women, 210 females were therefore selected for data analysis. The survey questionnaire was administered by the author. Prospective survey respondents were screened based on whether or not they had heard of Human Immunodeficiency Virus (HIV) or Acquired Immunodeficiency Syndrome (AIDS). A total of three female respondents had never heard of neither HIV nor AIDS, and were therefore excluded from the study. This study’s findings and analyses of female respondents' knowledge, perceptions, attitudes, and personal perceived risk of HIV/AIDS were, therefore, based on the remaining 207 female respondents. The survey questionnaire included items measuring respondents’ knowledge of HIV/AIDS transmission modes, perceptions and attitudes towards PLHIV and personal perceived risk of HIV/AIDS. There were 10 items to assess female respondents’ knowledge about HIV/AIDS (Cronbach’s Alpha = .83). Twelve items were designed to measure respondents’ perceptions of PLHIV and attitudes towards PLHIV respectively (Cronbach's Alpha = .72 for both). These items were plotted on a 5-point Likert scale; from strongly disagree to strongly agree. Three items, using dichotomous measurement ("agree" or "disagree"), assessed female respondents' personal perceived risk of HIV/AIDS. Data were recorded and analysed using the Statistical Package for the Social Science (SPSS 20.0). Statistical analysis included parametric statistics (i.e., Pearson correlation and T-test) and nonparametric statistics (i.e., frequencies, percentages, mean, and standard deviation).
4. RESULTS
4.1. Demographic Characteristics
Table 1 summarises the demographic characteristics of all 210 female participants for this study. Out of 210 female respondents, three of them have never heard about the disease. Thus, these people were excluded from the inferential data analysis but were retained for descriptive analysis. The table shows that the overall mean age of the female respondents was 29.31 years old (SD = 11.89). The majority of participants were Malays (53.8%), followed by Chinese (28.1%), Indians (13.8%) and others—consist of indigenous—was 4.3%. More than half of the respondents were Muslims with 56.2% and another 43.8% were non-Muslims. Ninety-one percent of the female respondents had higher education (minimum SPM level) while 9% of the female respondents had lower education.
Table-1. Socio-demographic characteristics
| Variable | Parameters | N | (%) |
| Age | Mean ± SD | 29.31 ± 11.89 | |
| Ethnicity | Malay | 113 | 53.8 |
| Chinese | 59 | 28.1 | |
| Indian | 29 | 13.8 | |
| Others | 9 | 4.3 | |
| Religion | Islam | 118 | 56.2 |
| Buddhist | 34 | 16.2 | |
| Taoist/Confucianism | 8 | 3.8 | |
| Hindu | 25 | 11.9 | |
| Christian | 20 | 9.5 | |
| Catholic | 2 | 1 | |
| Others | 3 | 1.4 | |
| Education Level | Lower | 19 | 9 |
| Higher | 191 | 91 |
Table-2. The response of modes of HIV/AIDS transmission
| Way of Transmission | Disagree | Agree | Neutral |
| Sex contact without proper protection (heterosexual or homosexual) | 9 (4.4) |
195 (93.2) |
5 (2.4) |
| Skin contact (hug or shake hands) | 174 (84) |
15 (7.2) |
18 (8.7) |
| Kissing | 93 (45) |
64 (30.9) |
50 (24.2) |
| Cough/sneeze | 115 (55.6) |
42 (20.3) |
50 (24.2) |
| Bites of flies/mosquitoes/other insects | 103 (49.8) |
66 (31.8) |
38 (18.4) |
| Sharing foods or drinks | 120 (58) |
47 (22.7) |
40 (19.3) |
| Sharing clothing | 149 (72) |
18 (8.7) |
40 (19.3) |
| Sharing utensils (e.g., spoon, cup, fork, etc.) | 113 (54.6) |
45 (21.7) |
49 (23.7) |
| Pregnancy | 25 (12.1) |
143 (69.1) |
39 (18.8) |
| Living/working with a person who has AIDS | 153 (73.9) |
26 (12.6) |
28 (13.5) |
Note: N=207, excluded the three respondents who have never heard about HIV/AIDS. Figures in parentheses represent percentages.
4.2. Knowledge of Modes of HIV/AIDS Transmission
Overall, over 90 percent of respondents were aware of HIV/AIDS transmission modes. Table 2 indicates most of the surveyed respondents agreed HIV can be transmitted through unprotected sexual intercourse (93.2%) and pregnancy (69.1%). However, misconceptions existed among some who believed that HIV/AIDS can be transmitted via skin contact (7.2%), kissing (30.9%), cough/sneeze (20.3%), bites from mosquitoes or other insects (31.8%), sharing foods or drinks (22.7%), sharing clothing (8.7%) and sharing utensils (21.7%).
4.3. Perception towards People Living with HIV/AIDS (PLHIV)
Respondents strongly believed that people living with HIV/AIDS (PLHIV) still have the ability to work (77.3%). However, 63.7% agreed that people living with HIV/AIDS should be isolated from other people. Seventy-two percent of the surveyed female respondents concurred that having HIV/AIDS is not an issue to be ashamed of. Sixty-eight percent of the respondents agreed that PLHIV is dirty. More than 50 percent of the respondents (54.1%) disagreed PLHIV should not have children. In other words, PLHIV should have children. As far as stigma and discrimination are concerned, 68.6% of the surveyed respondents still thought PLHIV should be blamed for bringing the disease into the community. In general, the surveyed female respondents held moderate positive perceptions towards PLHIV at M = 3.60 (SD = .60).
4.4. Attitude towards People Living with HIV/AIDS (PLHIV)
Notwithstanding moderate positive perceptions harboured among female respondents towards PLHIV, this survey’s results indicated that respondents had a discriminatory attitude towards PLHIV (M = 3.36, SD = .58). Specifically, 53.1% of the surveyed respondents were willing to work with PLHIV if they are asked to do so. However, more than fifty percent of the respondents would keep away from their close friends or kin if they were people living with HIV/AIDS (63.3%). In Malaysia, openly discussing HIV/AIDS is still a taboo subject (Tham and Zanuddin, 2015 ![]() ). As expected, 73% of the respondents refused to talk to friends or family members about HIV/AIDS-related issues. Only 42% of the respondents were willing to buy foods from vendors or shopkeepers who are PLHIV and 27% would be willing to have a meal with them. As expected, as stigma and discrimination are pervasive within the general population, less than half of respondents (29%) were willing to let others know if one of their friends or family members was infected with HIV.The researchers further analysed if there is a correlation between the surveyed respondents’ perceptions and attitudes towards PLHIV. Table 3 shows a positive correlation between the surveyed female respondents’ perceptions and attitudes towards PLHIV (r = .436, p=<.05). Although the result showed a weak correlation between the variables (Chua, 2013
). As expected, 73% of the respondents refused to talk to friends or family members about HIV/AIDS-related issues. Only 42% of the respondents were willing to buy foods from vendors or shopkeepers who are PLHIV and 27% would be willing to have a meal with them. As expected, as stigma and discrimination are pervasive within the general population, less than half of respondents (29%) were willing to let others know if one of their friends or family members was infected with HIV.The researchers further analysed if there is a correlation between the surveyed respondents’ perceptions and attitudes towards PLHIV. Table 3 shows a positive correlation between the surveyed female respondents’ perceptions and attitudes towards PLHIV (r = .436, p=<.05). Although the result showed a weak correlation between the variables (Chua, 2013 ![]() ) it indicated that the higher positive perception towards PLHIV one has, the higher positive attitude towards PLHIV of the person.
) it indicated that the higher positive perception towards PLHIV one has, the higher positive attitude towards PLHIV of the person.
Table-3. Relationship between perception and attitude towards people living with HIV/AIDS
| Perception | Attitude | |
| Pearson | 1 | .436** |
| Sig. (2-tailed) | 207 | .000 |
| N | 207 |
4.5. Personal Perceived Risk of HIV/AIDS Infection and Perception about Condom Use
This study shows that surveyed female respondents did not perceive to have the high risk of contracting HIV/AIDS, whereby 51.7% of the respondents did not think that they could be at risk of AIDS infection. While ABC approach (i.e., abstinence, being faithful to partners and condom use) is highly recommended by health practitioners and advocates in the effort of fighting HIV/AIDS, more than half of the female respondents (60.9%) agreed that they would protect themselves or their partners from contracting HIV/AIDS infection by using condoms and 71.5% of the respondents agreed that they can reduce their chances of contracting HIV/AIDS infection if they are being faithful to their partners/spouses.
In this study, the author found that there is a significant difference between Muslim and non-Muslim female respondents with regard to their perception towards the use of condoms in curtailing HIV/AIDS infection, t (202.08) = -2.642, p<.05. Muslim female respondents carried a mean score of 3.53 (SD = .1.12), while non-Muslim female respondents carried a mean score of 3.91 (SD = .99). The mean difference (M = -.386) indicated that non-Muslim female respondents were more likely to use condoms with their partners to protect themselves from contracting HIV/AIDS infection.
5. DISCUSSION
This study aimed to explore the knowledge, perceptions, attitudes and personal perceived risk of HIV/AIDS among women in Klang Valley, Malaysia. Several findings merit further consideration. The author can conclude that women in Malaysia are adequately knowledgeable about the modes of HIV/AIDS transmission. This finding is similar to Wong et al. (2008 ![]() )'s study, which they found that females were more knowledgeable than males about general HIV/AIDS knowledge. However, some misconceptions exist, wherein some surveyed respondents still believe that HIV/AIDS can be transmitted through mosquito bites, sharing utensils, foods or drinks and clothing. The significant increased awareness and knowledge about HIV/AIDS among women have given credit and supported efforts done by various parties such as the government, NGOs and the media in which they have successfully reached their target messages out to this population. Previous research have shown that stigma and discrimination related to HIV/AIDS have had profound effect on the lives of people living with HIV/AIDS, and acted as an obstacle to effective HIV prevention and treatment among these people (Majahan et al., 2008
)'s study, which they found that females were more knowledgeable than males about general HIV/AIDS knowledge. However, some misconceptions exist, wherein some surveyed respondents still believe that HIV/AIDS can be transmitted through mosquito bites, sharing utensils, foods or drinks and clothing. The significant increased awareness and knowledge about HIV/AIDS among women have given credit and supported efforts done by various parties such as the government, NGOs and the media in which they have successfully reached their target messages out to this population. Previous research have shown that stigma and discrimination related to HIV/AIDS have had profound effect on the lives of people living with HIV/AIDS, and acted as an obstacle to effective HIV prevention and treatment among these people (Majahan et al., 2008 ![]() ; Genberg et al., 2009
; Genberg et al., 2009 ![]() ; Tee and Huang, 2009
; Tee and Huang, 2009 ![]() ; Naing et al., 2010
; Naing et al., 2010 ![]() ). The present study found that moderate, rather than clear-cut positive perceptions and a discriminatory attitude towards PLHIV exist within women respondents who are reasonably knowledgeable about the modes of HIV/AIDS transmission. Essentially, women respondents think that people living with HIV/AIDS should be blamed for bringing the disease into the community. As a result of this blame-the-victim stigma, many PLHIV refuse to come forward for treatments. This unfair process of blaming-the-victim discourages people from serological testing, status disclosure, remaining in care and adhering to their treatment. This ultimately suggests that the level of receptivity among women towards PLHIV is somewhat low. So, the author suggests that gender relationships should be at the heart of communication strategies for HIV/AIDS prevention with the help of strong political will and media advocacy. The Condom King of Thailand, Mechai Viravaidya mentioned "If AIDS prevention and control is to work, it must be multi-sectoral. It is not a medical problem. It is a behavioural problem and any institution that can affect behavioural change must be involved" (D’Agnes, 2001
). The present study found that moderate, rather than clear-cut positive perceptions and a discriminatory attitude towards PLHIV exist within women respondents who are reasonably knowledgeable about the modes of HIV/AIDS transmission. Essentially, women respondents think that people living with HIV/AIDS should be blamed for bringing the disease into the community. As a result of this blame-the-victim stigma, many PLHIV refuse to come forward for treatments. This unfair process of blaming-the-victim discourages people from serological testing, status disclosure, remaining in care and adhering to their treatment. This ultimately suggests that the level of receptivity among women towards PLHIV is somewhat low. So, the author suggests that gender relationships should be at the heart of communication strategies for HIV/AIDS prevention with the help of strong political will and media advocacy. The Condom King of Thailand, Mechai Viravaidya mentioned "If AIDS prevention and control is to work, it must be multi-sectoral. It is not a medical problem. It is a behavioural problem and any institution that can affect behavioural change must be involved" (D’Agnes, 2001 ![]() ).
).
The media should also make specific voices of PLHIV visible on the media coverage so that the public will get to know these people more in hopes of eliminating stigma and discrimination on them. This study found that majority of the respondents do not think that they are at risk of HIV/AIDS infection. According to the Health Belief Model of behaviour change, individuals must perceive themselves to be at risk of the health threat, before they take actions to reduce risky behaviours or to engage in healthy alternative behaviour (Janz and Becker, 1984 ![]() ). Hence, Ndegwa et al. (2012
). Hence, Ndegwa et al. (2012 ![]() ) suggested that adolescents who report high perceived risk for HIV/AIDS practise safer sexual behaviours, whereas those who perceive low risk for contracting HIV/AIDS report practising unsafe sexual behaviours. The low perceived risk of HIV/AIDS among women in Malaysia may due to many people thought that AIDS is something abstract and it is not going to affect them. The author is of the view that the perception can be changed only if there is an appropriate medium which tells everything about the epidemic. Information-related HIV/AIDS should not only be disseminated throughout the at-risk population in inducing them to change their attitudes, behaviours, and perceptions about HIV/AIDS, but it is also should be targeted those who are not considering themselves at-risk. This study, therefore, provides base information and insight into outlining strategic communication plans to tackle this group who thinks they are not vulnerable to HIV/AIDS infection. While publicly promoting condom use in HIV/AIDS prevention is seemed to be contentious in Malaysia, the finding shows that high proportion of the surveyed respondents want to use condoms to protect themselves or their partners from contracting HIV/AIDS infection. Furthermore, the inferential statistical test indicates that there is a statistically significant difference between Muslim and non-Muslim respondents on their perceptions of the use of condoms in HIV/AIDS prevention, which non-Muslim respondents have higher receptivity of use of condoms in HIV/AIDS prevention compared to Muslim respondents. This shows a good sign where the Malaysian society has become more open in accepting the fact that condoms if used correctly and consistently, guarantee more than 90 percent effectiveness at preventing heterosexual acquisition and transmission of HIV/AIDS (Pinkerton and Abramson, 1997
) suggested that adolescents who report high perceived risk for HIV/AIDS practise safer sexual behaviours, whereas those who perceive low risk for contracting HIV/AIDS report practising unsafe sexual behaviours. The low perceived risk of HIV/AIDS among women in Malaysia may due to many people thought that AIDS is something abstract and it is not going to affect them. The author is of the view that the perception can be changed only if there is an appropriate medium which tells everything about the epidemic. Information-related HIV/AIDS should not only be disseminated throughout the at-risk population in inducing them to change their attitudes, behaviours, and perceptions about HIV/AIDS, but it is also should be targeted those who are not considering themselves at-risk. This study, therefore, provides base information and insight into outlining strategic communication plans to tackle this group who thinks they are not vulnerable to HIV/AIDS infection. While publicly promoting condom use in HIV/AIDS prevention is seemed to be contentious in Malaysia, the finding shows that high proportion of the surveyed respondents want to use condoms to protect themselves or their partners from contracting HIV/AIDS infection. Furthermore, the inferential statistical test indicates that there is a statistically significant difference between Muslim and non-Muslim respondents on their perceptions of the use of condoms in HIV/AIDS prevention, which non-Muslim respondents have higher receptivity of use of condoms in HIV/AIDS prevention compared to Muslim respondents. This shows a good sign where the Malaysian society has become more open in accepting the fact that condoms if used correctly and consistently, guarantee more than 90 percent effectiveness at preventing heterosexual acquisition and transmission of HIV/AIDS (Pinkerton and Abramson, 1997 ![]() ; Hearst and Chen, 2004
; Hearst and Chen, 2004 ![]() ). However, condom use is not necessarily the best means for HIV prevention from both religion and practical perspectives. Hence, practicing abstinence and fidelity are the most pragmatic approach for HIV/AIDS prevention.
). However, condom use is not necessarily the best means for HIV prevention from both religion and practical perspectives. Hence, practicing abstinence and fidelity are the most pragmatic approach for HIV/AIDS prevention.
6. LIMITATIONS
As far as methodological perspective is concerned, this research uses only the quantitative approach to study the women's knowledge, perceptions, attitudes and perceived risk of HIV/AIDS. From the post-positivism point of view, the author cannot observe the world in a purely objective way as people's perception is subjective. Due to that reason, it is recommended that a mixed method approach could be used in the future study in order to provide the future discourse of knowledge to exploring women’s views on HIV/AIDS-related issues. On top of that, items in measuring the knowledge of HIV/AIDS were designed on a 5-point Likert scale which is difficult to be computed into a single scale and correlate with other variables. Future research may, therefore, consider using dichotomous measurements such as "Ture" or False" in accessing knowledge of HIV/AIDS among surveyed respondents.
7. CONCLUSION
Sexual health could be critical to Malaysians. However, due to the strong social taboo against openly discussing sexual health-related issues (in this case, HIV/AIDS), it remains unclear to what extent Malaysians would consider sexual health-related issues relevant and how such perception would have an effect on their health decision making in the applied setting. As such, this study contributes to our understanding of Malaysian women's knowledge, perceptions, attitudes and perceived risk for HIV/AIDS. The results demonstrate that Malaysian women are generally knowledgeable on HIV/AIDS, but harbouring moderate perception and a discriminatory attitude towards people living with HIV/AIDS. The results expose the needs for more comprehensive education programmes. The contribution of this study is the inclusion of perceived risk or susceptibility as one of the variables to be tested among women. The author argues that the variable is very influential in prompting people to adopt healthier behaviours. The greater the perceived risk, the greater the likelihood of one engaging in behaviours to decrease the risk. Sadly, our results show that the surveyed women do not think that they are at risk of HIV/AIDS infection. This information is part and parcel for developing targeted and effective education programmes about HIV/AIDS among women in Malaysia.
REFERENCES
AIDS/STD Section, 2010. UNGASS country progress report: Reporting period January 2008 – December 2009. [Accessed 3 May 2018].
Allison, E.H. and J.A. Seeley, 2004. HIV and AIDS among fisherfolk: A threat to ‘responsible fisheries’? Fish and Fisheries, 5(3): 215-234. View at Google Scholar | View at Publisher
Alwafi, H.A., A.M.T. Meer, A. Shabkah, F.S. Mehdawi, H. El-haddad, N. Bahabri and H. Almoallim, 2018. Knowledge and attitudes toward HIV/AIDS among the general population of Jeddah, Saudi Arabia. Journal of Infection and Public Health, 11(1): 80-84. View at Google Scholar | View at Publisher
Bolan, G., A.A. Ehrhardt and J.N. Wasserheit, 1999. Gender perspectives and STDs. In Homes, K. K., Sparking, P. E., & Mardh, P. A. (Eds.). Sexually transmitted diseases. New York: McGraw-Hill Health Professions Division. pp: 117-127.
Centers for Disease Control and Prevention (CDC), 2001. First report of AIDS (Morbidity and Mortality Weekly Report). Retrieved from http://www.cdc.gov/mmwr/pdf/wk/mm5021.pdf [Accessed 3 May 2018].
Chua, Y.P., 2013. 2nd Edn., Basic research statistics: Analisis data scale likert [Basic Research Statistics: Analysis Likert Scale’s data]. Kuala Lumpur: McGraw-Hill.
D’Agnes, T., 2001. From condoms to cabbages: An authorized biography of Mechai Viravaidya. Bangkok: Post Books.
Dworkin, S.L., 2005. Who is epidemiologically fathomable in the HIV/AIDS epidemic? Gender, sexuality, and intersectionality in public health. Culture Health & Sexuality, 7(6): 615-623. View at Google Scholar | View at Publisher
Fauziah, M.N., S. Anita, N. Shaari, J. Ahamad, S. Pratap and A.K. Muhamad, 2002. HIV infection among fishermen in Terengganu. Malaysian Journal of Public Health Medicine, 2(1): 21-25.
Fox-Tierney, R.A., J.R. Ickovics, C.L. Cerrata and K.A. Ethier, 1999. Potential sex differences remain understudied: A case of inclusion of women in HIV/AIDS-related neuropsychological research. Review of General Psychology, 3(1): 44-54. View at Google Scholar | View at Publisher
Gebremedhin, S.A., W. Youjie and E.H. Tesfamariam, 2017. Predictors of HIV/AIDS knowledge and attitude among young women of Nigeria and democratic republic of Congo: Cross-sectional study. Journal of AIDS & Clinical Research, 8(3): 1-8. View at Google Scholar | View at Publisher
Genberg, B.L., Z. Hlavka, K.A. Konda, S. Mamanc, S. Chariyalertsak, A. Chingono and D.D. Celentano, 2009. A comparison of HIV/AIDS-related stigma in four countries: Negative attitudes and perceived acts of discrimination towards people living with HIV/AIDS. Social Science & Medicine, 68(12): 2279-2287.View at Google Scholar | View at Publisher
Guinan, M.E. and A. Hardy, 1987. Epidemiology of AIDS in the United States, 1981 through 1986. Journal of the American Medical Association, 257(15): 2039-2042.View at Google Scholar | View at Publisher
Hazarika, I., 2010. Knowledge, attitude, beliefs and practices in HIV/AIDS in India: Identifying the gender and rural-urban differences. Asian Pacific Journal of Tropical Medicine, 3(10): 821-827. View at Google Scholar | View at Publisher
Hearst, N. and S. Chen, 2004. Condom promotion for AIDS prevention in the developing world: Is it working? Studies in Family Planning, 35(1): 39-47. View at Google Scholar | View at Publisher
Higgins, J.A., S. Hoffman and S.L. Dworkin, 2010. Rethinking gender, heterosexual men, and women’s vulnerability to HIV/AIDS. American Journal of Public Health, 100(3): 435-445.View at Google Scholar | View at Publisher
HIV/STI Section, 2015. Global AIDS response progress: Report Malaysia 2015. Retrieved from http://www.unaids.org/sites/default/files/country/documents/MYS_narrative_report_2015.pdf [Accessed 15 May 2018].
Huang, M., 2002. HIV/AIDS among fishers: Vulnerability of their partners. In Williams, M. J., Chao, N. H, Choo, P. S., Matics, M. C., Nandeesha, M. Shariff, E., Tech, & Wong, J. M. C. (Eds.), Global symposium on women in fisheries: Sixth Asian fisheries forum. Kaohsiung, Taiwan, Penang: World Fish Center. pp: 43-53.
Janz, N.K. and M.H. Becker, 1984. The health belief model: A decade later. Health Education Quarterly, 11(1): 1-47. View at Google Scholar | View at Publisher
Joint United Nations Programme on HIV/AIDS, 2017. When women lead change happens. Retrieved from http://www.unaids.org/sites/default/files/media_asset/when-women-lead-change-happens_en.pdf [Accessed 3 May 2018].
Kamb, M.L. and P.M. Wortley, 2000. Human immunodeficiency virus and AIDS in women. In Goldman, M., & Hatch, M. (Eds.), Women and health. San Diego, CA: Academic Press. pp: 336-351.
Kelantanese Women top List of those Infected with HIV/Aids, 2010. The sundaily. Retrieved from http://www.thesundaily.my/node/135509 [Accessed 4 May 2018].
Kissling, E., E.H. Allison, J.A. Seeley, S. Russell, M. Bachmann, S.D. Musgrave and S. Heck, 2005. Fisherfolk are among groups most at risk of HIV: Cross-country analysis of prevalence and number infected. AIDS, 19(17): 1939-1946. View at Google Scholar | View at Publisher
Krejcie, R.V. and D.W. Morgan, 1970. Determining sample size for research activities. Educational and Psychological Measurement, 30(3): 607-610. View at Google Scholar | View at Publisher
Majahan, A.P., J.N. Sayles, V.A. Patel, R.H. Remien, D. Ortiz, G. Szekeres and C.T. J., 2008. Stigma in the HIV/ADS epidemic: A review of the literature and recommendations for the way forward. AIDS, 22(2): S67-S79. View at Google Scholar | View at Publisher
Mane, P. and S.A. Maitra, 1992. AIDS prevention: The socio-cultural context in India. Mumbai: Tata Institute of Social Sciences.
Mastro, T.D. and D. Kitayaporn, 1998. HIV type 1 transmission probabilities: Estimates from epidemiologic studies. AIDS Research and Human Retroviruses, 14(3): S223-S227. View at Google Scholar
Mohd S. B., G. Subramaniam and P.L. Tan, 2013. Awareness and vulnerability to HIV/AIDS among young girls. Procedia – Social and Behavioural Sciences, 105: 195-203. View at Google Scholar | View at Publisher
Mondal, M.N.I. and M. Shitan, 2013. HIV/AIDS epidemic in Malaysia: Vulnerability and risk of women. Asian Journal of Humanities and Social Studies, 1(5): 274-283. View at Google Scholar
Munusamy, S. and K.S. Fadzil, 2017. HIV/AIDS infection among Indian-Malaysian women: Sociological vulnerabilities and implication for family socio-economic development. Journal of Social Sciences and Humanities, 12(2): 183-195.
Mutombo, N. and B. Maina, 2015. Factors influencing attitudes towards people living with HIV/AIDS in Zambia: Does HIV testing matter? Journal of Infectious Diseases & Therapy, 3(1): 1-7. View at Google Scholar | View at Publisher
Naing, C.M., M. Hakim, D. A. T. Yee, R.M. Koo, C.Y. Tan, K.J. Kong and S.S.K. Siew, 2010. HIV/AIDS-related knowledge, attitudes and perceptions: A cross-sectional household survey. Southeast Asian Journal of Tropical Medicine Public Health, 41(4): 952-960. View at Google Scholar
Najimudeen, M. and M. M. Rosy, 2011. More HIV infection among housewives than sex workers in Malaysia. WebmedCentral Public Health, 2(2): 1-8. View at Google Scholar
Ndegwa, N., M.P. Wanderi and A. Mwisukha, 2012. Factors influencing behaviour change for the prevention of the spread of HIV/AIDS among students in Githunguri Division, Githunguri District, Kiambu County, Kenya. International Journal of Business and Social Science, 3(16): 313-324. View at Google Scholar
Nicolosi, A., M.L. Correa Leite, M. Musicco, C. Arici, G. Gavazzeni and A. Lazzarin, 1994. The efficiency of male-to-female and female-to-male sexual transmission of the human immunodeficiency virus: A study of 730 stable couples. Italian study group on HIV heterosexual transmission. Epidemiology, 5(6): 570-575. View at Google Scholar | View at Publisher
Padian, N., S.C. Shiboski and N.P. Jewell, 1991. Female-to-male transmission of human immunodeficiency virus. Journal of the American Medical Association, 266(12): 1664-1667.View at Google Scholar | View at Publisher
Pinkerton, S.D. and P.R. Abramson, 1997. Effectiveness of condoms in preventing HIV transmission. Social Science & Medicine, 44(9): 1303-1312. View at Google Scholar | View at Publisher
Royce, R.A., A. Sena, W. Cates and M.S. Cohen, 1997. Sexual transmission of HIV. New England Journal of Medicine, 336(15): 1072-1078. View at Google Scholar | View at Publisher
Samsudin, N., A. Ali, M.A.M. Aris, S. Draman and S.F.U.A. Akter, 2011. Social and HIV/AIDS risk behaviours in a fishing community. International Journal of Humanities and Social Science, 1(21): 251-257. View at Google Scholar
Singhal, A. and E.M. Rogers, 2003. Combating AIDS communication strategies in action. New Delhi: Sage Publications.
Tafazoli, M., M. Larki, R.L. Roudsari, M.T. Shakeri and A. Babaee, 2016. AIDS risk perception and its related factors in women with high-risk behaviours in Iran. Journal of Midwifery and Reproductive Health, 4(2): 582-591. View at Google Scholar
Tee, Y. and M. Huang, 2009. Knowledge of HIV/AIDS and attitudes towards people living with HIV among the general staff of a public university in Malaysia. Journal of Social Aspects of HIV/AIDS, 6(4): 179-187.View at Google Scholar | View at Publisher
Tham, J.S. and H. Zanuddin, 2015. Religion and media: A case study of Utusan Malaysia’sresponse to HIV/AIDS. Continuum, 29(1): 121-133. View at Google Scholar | View at Publisher
U.S. Department of Health and Human Services, 2001. First report of AIDS. Morbidity and Mortality Weekly Report, 50: 429-222.
United Nations Children’s Fund, 2008. Women and girls: Confronting HIV and AIDS in Malaysia. Retrieved from http://www.unicef.org/malaysia/Women_and_AIDSReport2008(1).pdf [Accessed 3 May 2018].
Wagbara, M., 2017. Gender inequality in women’s knowledge and awareness of HIV/AIDS in Port Harcourt. Doctoral Dissertation, Walden University.
Wan P.E., M. Jihad, J. Mustafa, B. Basuki and N. Ahmad, 2012. Knowledge, attitude and practice about HIV/AIDS and its influencing factors among pregnant mothers in West of Sabah Malaysia. Malaysian Journal of Public Health Medicine, 12(2): 15-23. View at Google Scholar
Women’s Aid Organisation, 2001. HIV/AIDS prevention for women from a gender perspective. Retrieved from http://www.wao.org.my/news_details.php?nid=67&ntitle=HIV/AIDS+Prevention+for+Women+from+a+Gender+Perspective [Accessed 15 May 2018].
Wong, L.P., C.L.C. Kwong, W.Y. Low and N. Jaafar, 2008. HIV/AIDS-related knowledge among Malaysian young adults: Findings from a nationwide survey. Journal of the International AIDS Society, 10(6): 148.View at Google Scholar | View at Publisher
Wortley, P.M. and P.L. Fleming, 1997. AIDS in women in the United States: Recent trends. American Journal of Public Health, 278(1): 911-916. View at Google Scholar | View at Publisher
Zierler, S. and N. Kriger, 1997. Reframing women’s risk: Social inequalities and HIV infection. Annual Review of Public Health, 18(1): 401-436. View at Google Scholar | View at Publisher