




TRAUMA-INFORMED EDUCATION PRACTICE IN CAMBODIA

1,2,3Deakin University, Melbourne, Australia
ABSTRACT
There is limited evidence that specifically focuses on teachers’ use of trauma-informed approaches in their classrooms. Trauma models exist in resource rich countries and many have been developed by social workers, however information about implementation of these models in resource poor countries is missing in the literature. This study explores the trauma-informed practice of teachers, social workers and clinicians working with traumatized children at Hagar International Cambodia. The research used an interpretive descriptive methodology encompassing a qualitative approach to data collection. Ten individual interviews and one focus group discussion were conducted at Hagar’s Phnom Penh school and office locations. Fourteen individuals participated in the study. Findings indicate a convergence of trauma-informed themes, including encouragement and empowerment, behavior management strategies, collaboration and relationship with others, trauma challenges and healing from trauma. This article explores Hagar International Cambodia’s trauma-informed education model and the experiences of social workers and educators working with traumatized children.
Keywords:Cambodia Intergenerational trauma The trauma-informed classroom Healing trauma Social work
ARTICLE HISTORY: Received:1 February 2018, Revised:16 February 2018, Accepted:20 February 2018, Published:23 February 2018.
Contribution/ Originality:This study contributes to the existing literature body of trauma-informed practice in education. However, this is one of very few studies which have investigated a trauma-informed approach being utilized in a developing nation, by exploring the lived experiences of professionals working with traumatized children in Cambodia. The paper's primary contribution is in the findings of a convergence of trauma-informed themes.
1. INTRODUCTION
Trauma may constitute the greatest cause of underachievement in schools worldwide, making learning a challenge for affected children (Perry, 2007; Wyatt and Oliver, 2016). In resource rich countries trauma-informed practice in education is receiving attention as a way of responding to a range of trauma symptoms in the classroom (Downey, 2007; Zeigler, 2013; Fecser, 2015; Brunzell et al., 2015b). It is important to identify how such practices are conceptualized and implemented not only in teaching and learning environments, but also for social workers, health professionals and other advocates of social justice (Walkley and Cox, 2013). The impact of trauma on children and youth is complex, effecting their education, general and mental health and their ability to develop trusting relationships with others (Wyatt et al., 2017).
This project explored how Hagar International Cambodia (hereafter ‘Hagar’) has implemented a Western trauma-informed model in their Phnom Penh school. Hagar delivered trauma-informed training to their primary school teachers in October 2015. This paper reports on a research project conducted over a six week period in early 2016, that explores trauma-informed practice with 14 individuals working in the Community Learning Centre (CLC), Hagar’s ‘catch up’ school in Phnom Penh,. Participants include teachers, social workers and clinicians who work with traumatized children on a daily basis.
Hagar provides services for women and children who are survivors of human rights abuse. Operating in Cambodia, Vietnam and Afghanistan, Hagar’s mission is to restore the lives of woman and children, by “walking the entire journey of recovery” – through recovery shelters, legal support, education and employment programs, health care, trauma counseling, and transitional and reintegration support (Hagar International, 2015). Hagar has been operating in Cambodia for over 20 years and has seen some of their children successfully complete their education and go on to University. This is a significant achievement, as many of these students have experienced considerable trauma in their young lives. Across all levels of the organization, Hagar’s work with victims of human trafficking is informed by social work values of empowerment and social justice s. This project looked at two groups of professionals working at Hagar: educational staff and clinical staff, which included social workers and management responsible for developing Hagar’s trauma-informed classroom model. Social work values of participation, empowerment, human rights and social justice underpin the anti-oppressive and strengths-based practices embedded within the organization. Therefore, Hagar Cambodia is in a unique position to demonstrate how social work may inform educational practices and highlights the nexus between these two disciplines.
Popper (1965) called for inter-professional collaboration between education and social work and stated that without it, the two sets of professionals will be “forced to learn more about one another’s process but in a diffused and ad-hoc manner” (cited in Bronstein and Abramson (2003)). Recently, there has been significant research into successful collaborations between teachers and social workers in multidisciplinary teams (Bronstein and Abramson, 2003; Berzin et al., 2011; Hesjedal et al., 2015). Ko et al. (2008) looked at creating trauma-informed systems around a child, drawing on evidence-based practice. Trauma may confront schools with serious dilemmas, such as how to balance their primary mission of educating students with the reality that many students need help to deal with traumatic stress so they can engage in learning (Ko et al., 2008). Many argue that social workers and teachers have a shared mission to help children and this common service fosters the development of interdisciplinary collaboration (Bronstein and Abramson, 2003). Research conducted by Berzin et al. (2011) found that practices that inform teachers’ understanding of trauma and utilize mental health professionals to support teachers, can “enhance students’ behavioral outcomes and improve learning”(p.500).
2. THEORETICAL BACKGROUND
Early trauma-informed research emerged in the 1970s and compared post-mortem autopsy analyses of brain changes, with clinical histories of child maltreatment prior to death (Delima and Vimpani, 2011). However, this method focused on major structural changes in the brain that occurred as a result of trauma (De Bellis et al., 2010). Specifically, children with no known maltreatment histories do not display the same brain structural changes apparent in cases of childhood maltreatment (De Bellis et al., 2002). More recently, assessments using a combined MRI-psychosocial approach found that the impact of maltreatment on a child’s brain can affect structural and functional changes which have been corroborated with observations about the children’s behaviors and cognitive functioning (De Bellis et al., 2002; Perry, 2009). The earlier the onset and the longer the child is exposed to the trauma experience, the greater the impact on the child’s development (De Bellis et al., 2002). The studies demonstrate that the longer a child experiences repetitive and prolonged maltreatment that they recognize as potentially life threatening, the greater the harm on early brain development (Anda et al., 2005; Perry, 2009). Trauma produces serious self-regulation deficiencies in the brain, often classified as ‘affect dysregulation’ and includes hyper-arousal (fight/flight stress response) and disassociation (mentally going to a different place) (Downey, 2007; National Child Traumatic Stress Network (NCTSN), 2008).
There are several models that provide practical classroom strategies for teachers working with traumatized children in developed nations. For example, Bloom’s ‘Creating Sanctuary’ Model, looks at the classroom much like a therapeutic community and proposes that teachers create a classroom environment that is trauma-sensitive by being ‘trauma-organized’, redirecting the trauma-scenario (repetition of behaviors) and self-destructive habits, by changing the direction of play (Bloom, 1995). The NCTSN (2008) Complex Trauma Taskforce built on Bloom’s work with the ARC Model (attachment, regulatory, competencies). Contemporary international trauma-informed models draw on the work of Bruce Perry and The Child Trauma Academy and focus on the impact of trauma on the neurodevelopment of a child’s brain (Perry, 2007; Perry, 2009). All the models propose ways to teach children to self-regulate focusing on the teacher-student relationship. For example, using rhythm and repetition in classroom activities to respond to affect-dysregulation, which is marked by heightened fluctuation of emotional responses. A teacher may use rhythm and repetition to diffuse a situation and/or encourage a child to develop a self-regulatory process of their own (Bloom, 1995; Downey, 2007; NCTSN, 2008).
2.1. Social Work Perspectives
Social work has critiqued the dominance of the medical model in response to trauma, arguing that the wider context of clients’ lives is largely neglected because the hegemonic medical paradigm is wedded to traditional psychiatry (Westoby and Ingmells, 2010; Knight, 2015; Quiros and Berger, 2015). This does not mean that social work rejects the medical model or neurodevelopmental approaches; instead it asserts that a range of knowledge is important to address the holistic needs of individuals and communities. Social workers argue that to become trauma-informed, a system must recognize trauma as both interpersonal and socio-political, and focus on fostering safety, respectful relationships, collaboration and empowerment at all levels of service delivery (Quiros and Berger, 2015). Publications by social workers in the field of trauma take into consideration the nexus between material circumstances, cultural context and diversity (Allan and Hess, 2010; Atkinson, 2013; Knight, 2015). They highlight that an effective trauma-informed approach needs to be informed by an understanding of neuropsychological cognitive functioning and also needs to draw on theories of empowerment, social connectedness, human rights and the structural factors associated with disadvantage and vulnerability to trauma. The Hagar trauma-informed model attempts to redress the injustice and rights violations experienced by their young students in ways that acknowledge and respond to the complexities of their experience through classroom practices aimed at restoring connection through relationships, and empowering students to develop their learning abilities.
2.2. Being ‘Trauma-Informed’ at Hagar
Hagar’s trauma-informed model demonstrates how teachers can view student behavior through the trauma lens, while trying to understand their feelings and thoughts, and by understanding behaviors as symptoms of their trauma history (Taylor, 2015). By participating in trauma-informed training, Hagar staff learns new language to describe students’ behaviors and new ways of responding in the classroom setting. Hagar’s model incorporates the social work focus of the person-in-environment (Taylor, 2015). For example, complex trauma is not understood by knowing ‘what happened’, rather by understanding the complexities of the trauma in relation to the lives of their clients. This approach moves away from a medical model, and instead considers a more holistic, strengths-based and contextual understanding of trauma. This approach acknowledges the historical and trans-generational trauma in Cambodia that has resulted from the Khmer Rouge Regime (1975-1979) and other factors that influence trauma such as gender, culture, age and developmental stage, personal characteristics, perception and problems faced following the trauma (Taylor, 2015). When teachers understand the complexities of trauma they are able to see beyond disturbed behaviors to create connections and diffuse conflict (Massachusetts Advocates for Children, 2005; Downey, 2007; Fecser, 2015). Change for these children is thought to come more easily if the focus extends beyond behavior management strategies to building connections, trust and stable relationships with significant adults (Wyatt and Oliver, 2016) often the most powerful reward for a child is the relationship between the adult and student. Research suggests that the most effective teachers display particular qualities such as: a calm demeanor; running a structured, predictable classroom; involving students in the lessons; demonstrating empathy; and understanding the functions of behavior (Anderson-Ketchmark and Alvarez, 2009; Szalavitz and Perry, 2010; Fecser, 2015).
The trauma-informed model used by Hagar was developed by an experienced expatriate social worker. The model allows teachers to develop an awareness of their students through a trauma lens, while at the same time understanding their student’s feelings, thoughts and behaviours as the symptoms of their trauma history (Taylor, 2015). The development of the model was informed by the work of American psychiatrists (Perry, 2007; Perry, 2009) and Siegel (2012) and draws on practical classroom models developed by Australian social worker Downey (2007) from Berry Street and The ACF (2010) model. The framework of the model is based on the work of Scottish social workers, Happer et al. (2006) and their understandings of how children in the child protection system can succeed in their studies.. This highlights the nexus between social work and trauma-informed education and emphasizes how social workers across the globe are informing classroom models and education practice with traumatized children.
2.3. Teachers’ Emotions and Self-Care
Knowledge about the victimization and maltreatment of children can be very distressing for educators and may produce feelings of anger, helplessness and hopelessness (Downey, 2007). Social workers are taught reflective practice and most engage in regular supervision to minimize stress and burnout. However, in a resource-poor school such as the Hagar’s CLC school, there may be little professional or personal support available, with some educators struggling to maintain personal boundaries alongside a sense of overwhelming responsibilities (Child Welfare Committee, 2008). Cole et al. (2013) discusses how educators and staff members who work with victims are also at risk of experiencing alterations in their feelings, their relationships and their thinking about the world, similar to the children themselves. Vicarious trauma, compassion fatigue, countertransference and secondary traumatic stress have been well researched in the social work profession (Kim and Kao, 2011; Diaconescu, 2015). Research analysing social worker burnout over the last decade, found that social workers working with trauma, “do not access the necessary resources to prevent and overcome secondary traumatic stress” (Diaconescu, 2015). It is likely that teachers working with trauma may experience a similar risk of burnout as the ‘burnout syndrome’ is more applicable to individuals possessing a high degree of enthusiasm to help others, in professions such as social, psychological and educational fields (Diaconescu, 2015). Relationships are a key resilience factor for traumatized children and may be just as important for the careers and professionals working with them. Research suggests that relational strategies such as expressing feelings and professional socialization with colleagues, supervisors and mentors, as well as doing activities together like cooking, eating and exercising are key strategies for coping with the adverse reactions of fatigue and secondary traumatic stress (Kim and Kao, 2011; Diaconescu, 2015).
It is essential that social workers and professionals in a variety of other sectors (eg. education, health, mental health) grasp the core concepts of how to best work alongside those who have experienced traumatic events in their lives to ensure sensitive and effective service delivery (Scott et al., 2010). It starts with an awareness that such problems exist, and then training to improve the capacity of those working alongside those who are traumatised so that survivors feel comfortable to share their stories and receive help. The underpinning research discussed in this section aligns with project aims and provides the framework for the exploration of Hagar’s trauma-informed approach. I think you need to connect your exploration of previous literature and research with your project here
3. METHODOLOGY
The overall aim of the study was: (a) to explore the impact of trauma-informed practice on classroom teaching and learning; and (b) to assess the self-care strategies and supports teachers’ utilize when working with traumatized children, and (c) highlight the practices that teachers use to manage student behavior and support the students to self-regulate their emotions and impulses during educational activities.. These aims were broken down further into the following objectives:
- Explore trauma-informed classroom practices teachers use to manage student behavior in the classroom;
- Identify how Hagar students are taught to self-regulate their emotions and impulses during educational activities in a classroom environment;
- Identify how Hagar teachers manage their own emotions to respond effectively to a child in a state of hyper-arousal/disassociation;
Identify challenges that teachers and social workers face in the implementation and maintenance of Hagar's trauma-informed classroom.
Interpretive description (ID) methodology (Thorne et al., 1997) is a non-categorical yet grounded approach to identifying themes and patterns that emerge in the context of health related phenomena. ID can be described as “an inductive analytic approach designed to create ways of understanding clinical phenomena that yield applications implications” (Thorne et al., 2004). This framework and approach was selected because it is compatible with social work values of participation, empowerment and social justice and seeks to understand human actions, recognizing and explaining the social context by discussing ambiguities, with the ownership of knowledge belonging to participants (Hansen, 2006; Thorne, 2010). ID draws from a naturalistic and constructivist orientation, understanding that human experience is socially constructed and subjective, whilst acknowledging the opportunity for shared realities (Thorne et al., 1997). ID assumes that for multiple realities to exist, a holistic approach to inquiry is required and the researcher and researched must interact to co-create understandings (Hansen, 2006). The researcher conducted fieldwork over a six week period which provided an opportunity for multiple realities to emerge through face-to-face interviews with participants.
3.1. Anti-Oppressive Social Work Research Practice (AOSWRP)
Qualitative approaches emphasize human interpretation, inductive reasoning, holistic understanding, rich data and contextualized explanation (Hansen, 2006). Building on this, anti-oppressive research is not looking for one truth, rather it is looking for meaning and understanding embedded in people’s life experiences. From an anti-oppressive perspective ‘pure knowledge’ does not exist, it is produced through the interactions of people and is therefore socially located and constructed (Potts and Brown, 2008). Therefore, the AOSWRP paradigm fits with an ID qualitative approach to social work research. This is because an anti-oppressive framework for research fits within the organizational culture of a social work strengths-based, empowerment model used at Hagar and embedded in the research aims. Importantly, AOSWRP is not just the way in which research is carried out; it is also the emancipatory aim of the project. Social work embraces a distinct purpose: “the empowerment and liberation of people to enhance wellbeing” and opposes the roots and effects of social oppression (Australian Association of Social Workers (AASW), 2010). Strier (2006) argues that in order to achieve the emancipatory purpose of the social work profession, research should defy traditions of social science research, which can reduce the research process to mere technical evaluations.
The Focus Group Discussion (FGD) involved Hagar’s social workers and other members of Hagar’s clinical team, who were responsible for the development and delivery of the trauma-informed classroom strategies. This provided initial context for the project and incorporated some of the more clinical trauma-informed language and knowledge, while aiming to give voice to all participants working with traumatized children using the trauma-informed model. Eight interviews with school teachers and staff at Hagar’s CLC were conducted using semi-structured open-ended questions, providing room for active participation. Two further interviews were conducted with senior management who are both social workers and tasked with overseeing Hagar operations in Cambodia. The FGD was to set the scene and add context to the following interviews, as it contained members of the clinical team who had been responsible for developing and providing the trauma-informed training to the educational arm at Hagar.
Sample Questions
| Focus Group Discussion Example Questions | Individual Interviews Example Questions |
|
1. Give me an example of a really good day at the school, what do you think the teachers do well? 2. Thinking about the school, what’s working well? 3. I understand the teachers recently finished TI training, have you seen any differences in the way they work with the children? 4. Is it different to what they were doing before? 6. Give me an example of a difficult day that the teachers have with children 7. What is a difficult/challenging day for you? 8. What are some of the behaviors that children exhibit? 9. How are the teachers managing those behaviors? 10. What would make it easier for the teachers? 11. On a good day, how do you celebrate your achievements? On a bad day, what do you do to make yourself feel better? |
1. What do you like about your work with children? 2. Give me an example of a really good day 3. When working with children, what do you think you do well? 4. I understand you finished some training in October, have you changed what you do in the classroom since completing the training? 5. Is it different to what you were doing before? 6. Give me an example of a difficult day with some of the children. How did you manage the situation? 8. How did you help the child/children feel calmer and be able to go back to learning? 9. Were you able to use anything from the training to help the child? 10. What would make your work easier? 11. On a good day, how do you celebrate your achievements? On a bad day, what do you do to make yourself feel better? |
A flyer was used to recruit participants and the purpose and details of the study was also mentioned by insiders at prospective teacher and clinical staff meetings. Member checking was conducted by emailing participants their transcripts to allow them to review the manuscript and provide additional information. In addition, a meeting was arranged with each participant to give them an additional printed copy of their transcript to check for accuracy in the transcription. This anti-oppressive qualitative research approach enhances the research process allowing substantive theory to emerge from the data where the voices of participants are central (Hansen, 2006; Marlow, 2011; Rodgers, 2012).
Hagar employs 86 staff in Cambodia, both in Phnom Pehn and throughout the provinces. The focus of this research was the clinical team responsible for the trauma-informed program and the teachers and school staff at CLC who were creating a trauma-informed space within the school. Both groups are located in Phnom Penh and account for almost half of Hagar’s total staffing. Invitations to participate were specifically targeted to these two groups and participants volunteered for the study. Early context for the project was provided by management and the clinical team and then further explored in one-on-one interviews with educational staff. The table below provides the participant characteristics. The participants highlighted in blue took part in the FGDs while the others participated in interviews.
Table-1. Participant characteristics
| Age | Gender | Education qualifications | Profession | Employed at Hagar since: |
| 62 | F | BA in Education + Masters in Social Work | Psychosocial Capacity Building Advisor | 2005 |
| 30 | M | BA in Psych + Masters | Senior Counsellor | 2009 |
| 32 | M | BA in Psych + Masters | Boys Counsellor | 2009 |
| 29 | M | BA in English Literature | Admin & Translation Advisor | 2012 |
| 44 | M | Undergrad & Masters in Social Work | Country Manager | 2012 |
| 34 | M | BA in Education + Masters | CLC Principal | 2010 |
| 35 | F | BA in Management + Diploma of Counselling | Senior Counsellor | 2010 |
| 44 | F | BA in Education | Primary Teacher | 2001 |
| 31 | F | Workplace Training | Primary Teacher | 2007 |
| 58 | M | BA in Education | Primary Teacher | 2007 |
| 52 | M | BA in Education | Primary Teacher | 2005 |
| 35 | F | BA in Accounting + TESOL | English Teacher | 2006 |
| 45 | M | BA in Education | Primary Teacher | 2010 |
| 29 | F | BA in Management Information Systems | Librarian | 2008 |
3.2. Data Analysis and Coding
The early stage analysis of ID focuses on big picture questions such as “what is happening here?” and “what am I learning about this?” (Thorne, 2010). The interview transcripts that were recorded in Khmer were transcribed back into English and then read multiple times before coding commenced, creating links and themes within the data (Saldana, 2014). This enabled intimate knowledge of each experience from which common themes were identified (Thorne, 2010; Saldana, 2014). Major themes and sub-themes were identified using a color coding system and data was split and ‘lumped’ together, identifying commonalities in participant responses (Saldana, 2014). A ‘note to self’ method was used to help move the analysis forward by recording emerging themes (Hansen, 2006). Five key themes emerged (see Table 2) and the will be discussed in the Findings.
Table-2. Key themes and sub-themes
| Theme 1 | Encouragement / Empowerment Sub-themes: language (verbal & non-verbal), sweet words, acknowledgement of good behaviour, repetitive instruction |
| Theme 2 | Behavioural Management Strategies Sub-themes: awareness/understanding of child stress, role modelling, behaviour modification techniques, trauma-informed strategies & persistence |
| Theme 3 | Relationship with Others Sub-themes: communication & relationship building between parents/teachers/counsellors, working with the child to create solutions, supervision & peer support |
| Theme 4 | Internal / External Challenges Sub-themes: poverty, hunger, collecting rubbish, problems at home, Intergenerational trauma, living conditions in the community, personal trauma experiences, budgets & funding restrictions, child behavioural issues & violence |
| Theme 5 | Self-Care and Healing from Trauma Sub-themes: love, hope, positivity, self-awareness, spirituality & religion as a resilience factor and how personal experiences enhance understanding |
3.3. Ethical Considerations
The researcher is a member of the Australian Association of Social Workers (AASW) and bound by the AASW Code of Ethics for culturally sensitive practice. Informed consent was obtained from individuals and Hagar. Approval was obtained by both Deakin University (where the researcher is a PhD student) Human Research Ethics Committee (DUHREC) and the Cambodian Ministry of Health (MoH) in December 2015. Additionally, several procedures were undertaken throughout the project in an effort to maintain confidentiality and anonymity of the participants in a small workplace such as Hagar. The invitation flyer, plain language statement, consent forms and information given verbally at staff meetings, highlighted the project aims, research activities, confidentiality and voluntary nature of the project (Potts and Brown, 2008). During transcription all participants were assigned a code name/number so data was not identifiable. The code ‘TSS’ is used to identify teachers and school staff, whilst the code ‘C’ stands for Clinical and is used to identify social workers and counselors.
4. FINDINGS
4.1. Encouragement and Empowerment
All teachers identified common emotionally-challenging behaviors, such as children being distressed, distracted, tearful, not coping, scared, angry and lashing out. Through the development of a trauma lens teachers understood that “every behavior tells a story” (C1 & C6), for example when a child acts out, either with anger towards others or “crying for no reason” (TSS8). Teachers frequently used multiple encouragement strategies to respond, such as: positive reinforcement, acknowledgement of good behavior, self-awareness of own mood in the co-regulation process, repetitive instruction and the use of language; including verbal, non-verbal and ‘sweet words’ to respond to a child in distress.
Many teachers used the term ‘sweet words’ when discussing encouragement and empowerment strategies. By sitting with the child and using positive reinforcement such as “you’ve done this before, you can do it again” (TSS3) and “we can do this together” (TSS7) a child focuses on their achievements and capabilities. Positive reinforcement for good behavior was identified by some teachers as setting children up with life skills for the future:
“Like a piece of paper that has been broken, we need to go backwards step by step and fill in where it is broken. We teach the children hope for the future so they might have a good life” (TSS6).
A link between teachers’ and students’ emotions was recognized. Many teachers talked about taking deep breaths and speaking in a soft tone, recognizing this co-regulation process as:
“When a teacher cannot control their emotions, the situation with the child always escalates” (C2).
Many teachers recognized and spoke about specific challenges relating to the impact of trauma on the brain, such as memory, concentration and learning difficulties. Teachers’ focused on encouragement, patience, repetitive instruction and movement to respond to these challenges:
“They are hard to teach as their brain is different, so you must give good advice again and again; spend a long time for advice” (TSS3).
“Sing, count the fingers, move the body, helps the brain” (TSS7).
4.2. Behaviour Management Strategies
Participants discussed the ‘trauma lens’ and it was evident that this concept resonated with the teachers, many of whom had been employed at Hagar for a long time:
“Using the trauma lens helps you understand emotions and behavior… I don’t wear black glasses when I look at the children, I wear pink glasses” (TSS2).
This is a significant shift, as the trauma-informed training appeared to give teachers further insight into what many of them had been seeing for a number of years:
“Instead of blaming or labeling the child, asking yourself: what is the child trying to tell me about their trauma?” (C1).
Participants talked about the specific trauma-informed behavior management strategy of a ‘time-in corner’ as opposed to a ‘time-out in isolation’ strategy sometimes employed in a classroom setting. Teachers recognized the labor-intensive nature of responding to traumatized children as they frequently needed more individual time and care than ‘normal’ students:
“We cannot talk meaningfully with children who are angry or sleepy. So we wait and make time to talk to them, we never shout” (TSS1).
Teachers also commented how students with trauma needed a lot of attention particularly as many of these students engaged in fighting, bullying and physical violence at the school.
"There are problems. It is not uncommon that they use violence and sexualized language learnt from home in the community” (C3).
"There are gender differences. Boys keep silent and fight, girls are scared and cry. This is hard to manage sometimes because there are so many of them" (TSS7).
Teachers felt they needed to spend time with the children modeling good behavior. According to one participant “ a lack of self-confidence, anxiety and lack of trust” (TSS7) was experienced by many of the children in regards to both their peers and other adults. Other participants commented that “time and persistence” was required to build bridges and “regain the trust” of the children (TSS4, TSS5). A member of the clinical team further commented that “counseling is not enough; they need to make friends and build relationships at school to learn how to trust again” (C6).
4.3. Interpersonal Workplace Relationships
The majority of teachers acknowledged the important work the clinical team did during the counseling sessions and noted that counselors helped the children “rebuild emotions” (TSS8) and “feel calm” (TSS6) so they can focus in class. However, there was a perception amongst some clinical team members that teachers may be resentful of them for “playing games with the children and earning more money” (C4). There was a perception held by a few teachers that it was “easier” to be a counselor as “they have one (child), we have 20” (TSS3).
The social workers and the counseling team have regular supervision and debriefing built into their work program, with one social worker commenting that “self-awareness and supervision” is the key when working with traumatized children (C1). There is an informal debriefing process in place, which also highlights the importance of supporting teachers working with trauma. Furthermore, participants commented on their regular informal morning teas as a self-care measure, citing humor and laughter as a way of supporting each other (TSS1, C6).
4.4. Internal and External Challenges
Most participants mentioned that external factors such as children living in poverty and the need to collect rubbish at night for their family’s economic survival compounded their learning difficulties. General living conditions in the community and intergenerational trauma were cited as ongoing challenges.
“Their houses may be flooding, or there is violence at home so they sleep on the streets and they don’t have any food” (TSS5).
“Trauma is not only rape and violence, its hunger and poverty too” (TSS8).
Social workers and clinicians spoke about the challenging behaviors in the classroom and considered that these behaviors were underpinned by feelings of worthlessness. They used words such as “disappointed with self”, “my family is bad”, “shy to others” and “feels dirty” (C2 and C3) to describe some of the emotional states their clients might be experiencing.
Participants also spoke about some of the challenges they faced when working with traumatized children; as many participants had experienced trauma themselves in early childhood. They commented that it was “hard” when they first started teaching as it reminded them of the trauma they had experienced (TSS7, TSS5 & TSS4). There were also the perceptions of others that provided challenges to the two disciplinary areas, with counselors commenting that:
“Teachers don’t really understand psychology well” (C4)
4.5. Healing from Trauma
Love, hope and spirituality were interwoven themes in the interviews. Even though there were no specific interview questions regarding religion and spirituality, the topic kept emerging in participants’ responses when asked about their self-care practices. One participant talked about love and sharing her ‘light’ with the children (TSS2) while another participant talked about finding hope in the Bible after a challenging day (TSS3). Participants were a mix of Buddhist and Christian yet it was evident in many interviews that spirituality played an important part in participants’ emotional wellbeing, with one commenting that "God and faith is very important for me. This is how I take care of my spirit" (C6). Similarly, other participants linked faith to feelings of calm and taking care of themselves emotionally:
“I go to church… sometimes I cry but I turn to Jesus for help” (C6).
"I go to the pagoda and I feel calm" (TSS4).
Love for the children was a common theme and many teachers identified them as the key to teaching traumatized children:
“The most important thing is that I give love. I speak slowly and gently and educate them to see the whole world as they think ‘oh my life is useless’, but if they have hope in their life they think ‘oh my future there might be good things in my life’, I give this education to them” (TSS2).
Teachers also expressed a strong sense of pride and job satisfaction, despite the challenges of working with trauma. Participants talked about various hobbies and activities they did together as a team, but also having some quiet time for reflection to renew their spirits and recharge emotionally, despite the challenges of working with trauma. Many talked about what made them happy and how proud they were to be making a difference in the children’s lives:
“At first they don’t want to talk to the teacher because he is a man... It takes time but now some of them call me papa” (TSS5).
“I am happy when they ask questions. When they ask questions, you know they are not scared anymore” (TSS2).
Many teachers said they enjoyed regular, informal, catch ups with other teachers and school staff over afternoon tea. More formal rewards and celebrations occur with teachers to recognize them for having the most students who reach their learning outcomes. Some discussed self-care strategies of “never taking work home” (TSS8).
5. DISCUSSION
Feeling emotionally safe is important for both children and staff. Several teachers discussed the personal distress experienced when a child would confide in them. However, instead of a ‘boundary trespass’ occurring where a teacher feels the need to ‘save’ a child (Bloom, 1995) an unexpected sub-context of spirituality emerged in the data, with many participants talking openly about their religious practice as a self-care measure. Downey (2007) acknowledges the distress teachers can feel when hearing about the maltreatment of a child, which in the long-term can put them at risk of vicarious trauma and compassion fatigue (Child Welfare Committee, 2008; Kim and Kao, 2011; Diaconescu, 2015). Other self-care strategies used by Hagar staff are their social connections, support of colleagues and the debriefing process in place. . This, as well as making time for hobbies and quiet reflection, highlights the importance of teachers finding something outside of work to renew their spirits and energy (Downey, 2007; Brunzell et al., 2015a). this needs to be clearly demonstrated in your findings through the data Section included about to demonstrate link
For the children, healing from trauma is contingent upon empowerment and the formation of new social connections with others (Wyatt and Oliver, 2016). Teachers spoke at length about love and trust they have with their students and drew parallels with their own children. As the literature suggests, the impact of abuse and neglect is seen in the developmental delays and social functioning of children, which can often mature into antisocial behaviour as adults and poor health outcomes (Szalavitz and Perry, 2010; Siegel, 2012). By understanding children’s emotional and physical states, Hagar teachers are using love and understanding to create a safe space for learning (Bloom, 1995). As the relationship between a child and their teacher can be one of the most powerful relationships that a trauma survivor will have in early recovery, it is often the stepping stone for learning how to trust again (Szalavitz and Perry, 2010).
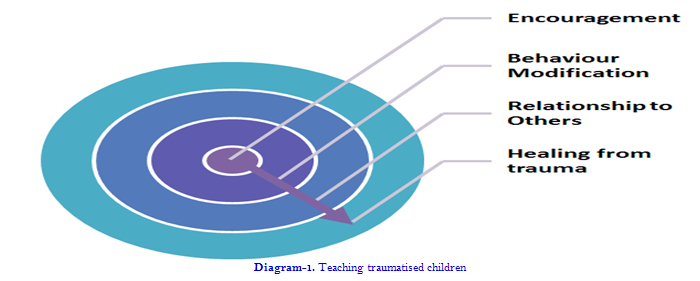
The themes outlined in the diagram below are sequential and interwoven and interconnected in a trauma-centered approach (Downey, 2007; Australian Childhood Foundation, 2010; Quiros and Berger, 2015). If encouragement is the key response from teachers and leads to behavioral change and a calmer classroom and school yard, then this is the place where a child is able to establish connections and build relationships essential for healthy socio-emotional development (Szalavitz and Perry, 2010). These relationships will enable a child to heal from trauma and grow into a functioning adult capable of self-control, trust, empathy and deep relational connections with others (Szalavitz and Perry, 2010).
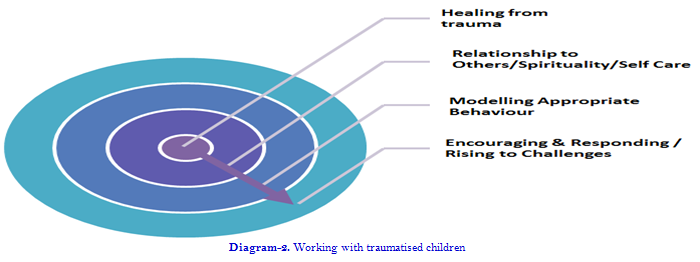
For professionals working with traumatized children, the themes are reversed in the next diagram, with healing and self-care at the center. Without this, a teacher may struggle to model appropriate behaviors and respond effectively to a class of hyper-vigilant children. Teachers spoke of the potential to be triggered on a personal level by a child and without appropriate self-care strategies and connection to others; the risk of secondary trauma and compassionate fatigue is likely to increase dramatically (NCTSN, 2008; Kim and Kao, 2011). Professionals who have not experienced trauma in early life are not immune to secondary trauma and still have to practice self-care. Whether this is spirituality, loving relationships with family or connection and laughter with colleagues, they are protective factors for working with trauma (Holloway and Moss, 2010; Friedman-Krauss et al., 2014; Hall and Souers, 2015; Hesjedal et al., 2015). It is fundamental when working with traumatized children that a professional remains calm and be at peace with themselves and the world around them, so they can respond effectively to a child in a state of hyper-arousal (Bloom, 1995; Downey, 2007; Brunzell et al., 2015b).
6. CONCLUSION
Models and curriculum strategies for schools working with a cohort of traumatized children exist in resource rich countries. Research in resource rich countries has shown that in order to support children exposed to trauma, a program is required that focuses on the self-regulation of emotions of both professionals and children, so that learning may take place (Bloom, 1995; Downey, 2007; NCTSN, 2008; Brunzell et al., 2015b). This research demonstrated that the Hagar teachers found being trauma-informed of benefit to their teaching practices, classroom management and understanding of themselves and their students. how did you demonstrate that in the findings??
6.1. Evident In Their Comments – Pink Glasses Etc
Teacher self-care embedded in spirituality can provide the basis for trauma-informed practice at Hagar. Teachers continually described their motivation and their practice using words such as ‘love’ and ‘encouragement’ stemming from a solid foundation of spirituality. Through this, teachers can best connect with love and care for the children in a way that empowers them with self-belief. Perhaps the most effective trauma informed practice is reliant on the use of the spiritual self that creates relationships that are safe, welcoming and supportive.
“Understanding someone’s suffering is the best gift you can give another person. The more you understand, the more you love; the more you love, the more you understand. They are two sides of one reality”. - Thich Nhat Hanh, Zen Buddhist Teacher (Hanh, 2014).
| Funding: This study received no specific financial support. |
| Competing Interests: The authors declare that they have no competing interests. |
| Contributors/Acknowledgement: All authors contributed equally to the conception and design of the study. |
REFERENCES
Allan, J. and L. Hess, 2010. The nexus between material circumstances, cultural context and experiences of loss, grief and trauma: Complexities in working with refugees in the early phases of resettlement. Grief Matters, 13(3): 76-80.View at Google Scholar
Anda, R.F., V.J. Felitti, J.D. Bremner, J.D. Walker, C. Whitfield and B. Perry, 2005. The enduring effects of abuse and related adverse experiences in childhood: A convergence of evidence from neurobiology and epidemiology. European Archives of Psychiatry and Clinical Neuroscience, 256(3): 174-186. View at Google Scholar | View at Publisher
Anderson-Ketchmark, C. and E.M. Alvarez, 2009. Addressing trauma in schools: An online resource. Children & Schools, 31(3): 189-191. View at Google Scholar | View at Publisher
Atkinson, J., 2013. Trauma-informed services and trauma-specific care for Indigenous Australian children. Closing the Gap Clearinghouse. Retrieved from http//www.aihw.gov.au/closingthegap .
Australian Association of Social Workers (AASW), 2010. Code of ethics. Australian Association of Social Workers. Retrieved from http://www.aasw.asn.au/document/item/1201
Australian Childhood Foundation, 2010. Making space for learning: Trauma informed practice in schools. Australian Childhood Foundation. Retrieved From:http://www.childhood.org.au/~/media/Files/Fundraising%20files/Fundraising%20resource%20files/Making%20space%20for%20learning%20ACF.ashx
Berzin, S., C. McManama-Obrien, A. Frey, M.S. Kelly, M.E. Alvarez and G. Shaffer, 2011. Meeting the social and behavioural health needs of students: Rethinking the relationship between teachers and school social workers. Journal of School Health, 81(8): 493-501. View at Google Scholar | View at Publisher
Bloom, S., 1995. Creating sanctuary in the school. Journal for a Just and Caring Education, 1(4): 403-433.View at Google Scholar
Bronstein, L.R. and J.S. Abramson, 2003. Understanding socialisation of teachers and social workers: Groundwork for the collaboration in the schools. Families in Society, 84(3): 323-330. View at Google Scholar | View at Publisher
Brunzell, T., J. Norrish, S. Ralston and M. Witter, 2015a. Berry street education model: Curriculum and classroom strategies. Richmond, VIC: Berry Street Victoria.
Brunzell, T., H. Stokes and L. Waters, 2015b. Trauma-informed positive education: Using positive psychology to strengthen vulnerable students. Contemporary School Psychology. Retrieved from http://link.springer.com/article/10.1007%2Fs40688-015-0070-x .
Child Welfare Committee, 2008. Child welfare trauma training toolkit: Comprehensive guide. 2nd Edn., Los Angeles, CA & Durham, NC: National Child Traumatic Stress Network.
Cole, F., A. Eisner, M. Gregory and J. Ristuccia, 2013. Helping traumatised children learn: Safe, supportive, learning environments that benefit all children. Massachusetts: Advocates for Children & Harvard Law School.
De Bellis, M.D., S.R. Hooper, D.P. Woolley and C.E. Shenk, 2010. Demographic, maltreatment and neurobiological correlates of PTSD symptoms in children and adolescents. Journal of Paediatric Psychology, 35(5): 570–577. View at Publisher
De Bellis, M.D., M.S. Keshavan, H. Shifflett, S. Iyengar, S.R. Beers, J. Hall and G. Moritz, 2002. Brain structures in paediatric maltreatment-related posttraumatic stress disorder: A socio-demographically matched study. Biological Psychiatry, 52(11): 1066–1078. View at Google Scholar | View at Publisher
Delima, J. and G. Vimpani, 2011. The neurobiological effects of childhood maltreatment: An often overlooked narrative related to long-term effects of early childhood trauma? Australian Institute of Family Studies, 89: 42-52. View at Google Scholar
Diaconescu, M., 2015. Burnout, secondary trauma and compassionate fatigue in social work. Social Work Review, 14(3): 57-63. View at Google Scholar
Downey, L., 2007. Calmer classrooms: A guide to working with traumatised children. Child safety commissioner. Victorian Government. Retrieved from http:// www.ccyp.vic.gov.au/childsafetycommissioner/downloads/calmer_classrooms.pdf.
Fecser, M.E., 2015. Classroom strategies for traumatized, oppositional students. Reclaiming Children and Youth, 24(1): 20-24. View at Google Scholar
Friedman-Krauss, A., C. Raver, P. Morris and S. Jones, 2014. The role of classroom-level child behaviour problems in predicting preschool teacher stress and classroom emotional climate. Early Education and Development, 25(4): 530-552.View at Google Scholar | View at Publisher
Hagar International, 2015. Where We Work: Cambodia. Retrieved from https://hagarinternational.org/international/our-work/where-we-work/cambodia/.
Hall, P. and K. Souers, 2015. Addressing trauma with calm, consistent care Principal, 94(4): 14-17.
Hanh, N.T., 2014. How to love: Mindful essentials. New York: Parallax Publishing.
Hansen, E.C., 2006. Successful qualitative health research: A practical introduction. Crows Nest, NSW: Allen & Unwin.
Happer, H., J. McCreadie and J. Aldgate, 2006. Celebrating success: What helps looked after children succeed. Social Work Inspection Agency. Retrieved from http://www.gov.scot/Resource/Doc/129024/0030718.pdf.
Hesjedal, E., H. Hetland and A.C. Iversen, 2015. Inter-professional collaboration: Self-reported successful by teachers and social workers in multidisciplinary teams. Child and Family Social Work, 20(4): 437-445.View at Google Scholar | View at Publisher
Holloway, M. and B. Moss, 2010. Spirituality and social work. Basingstoke, UK: Palgrave Macmillan.
Kim, H.J. and D. Kao, 2011. Burnout and physical health among social workers: A three-year longitudinal study. Social Work, 53(3): 258-268. View at Google Scholar | View at Publisher
Knight, C., 2015. Trauma-informed social work practice: Practice considerations and challenges. Clinical Social Work Journal, 43(1): 25-37. View at Google Scholar | View at Publisher
Ko, S.J., N. Kassam-Adams, C. Wilson, J.D. Ford, S.J. Berkowitz and M. Wong, 2008. Creating trauma-informed systems: Child welfare, education, first responders. Health Care, Juvenile Justice. Professional Psychology Research and Practice, 39(4): 396-404. View at Google Scholar | View at Publisher
Marlow, R.C., 2011. Research methods for generalist social work. 5th Edn., Belmont, CA: Brooks/Cole Cengade Learning.
Massachusetts Advocates for Children, 2005. Helping Children Learn. MAC August 2015. Retrieved from http://traumasensitiveschools.org/tlpi-publications/download-a-free-copy-of-helping-traumatized-children-learn/
National Child Traumatic Stress Network (NCTSN), 2008. Child welfare Trauma training toolkit. NCTSN Complex Trauma Taskforce. Retrieved from http://www.nctsn.org/products/child-welfare-trauma-training-toolkit-2008.
Perry, B., 2007. Bonding and attachment in Maltreated children: Consequences of emotional Neglect in childhood. The Child Trauma Academy. Retrieved from http://www.cpri.ca/uploads/section000181/files/bonding%20and%20attachment%20in%20maltreated%20children.pdf [Accessed 15 August 2015].
Perry, B., 2009. Examining child maltreatment through a neurodevelopmental lens: Clinical applications of the neurosequential model of therapeutics. Journal of Loss and Trauma, 14(4): 240-255. View at Google Scholar | View at Publisher
Popper, 1965. The challenge of the two professions. in R.H, Beck, ed, Society and the schools: Communication challenge to education and social work. New York: NASW Press. pp: 161-172.
Potts, K. and L. Brown, 2008. Becoming an anti-oppressive researcher. In Rethinking Society in the 21st Century: Critical Readings in Sociology, Webber M., & Bezanson, K. Eds. Toronto, Canada: Canadian Scholars’ Press. pp:50–57.
Quiros, L. and R. Berger, 2015. Responding to the sociopolitical complexity of trauma: An integration of theory and practice. Journal of Loss & Trauma: International Perspectives on Stress and Coping, 20(2): 159-159.View at Google Scholar | View at Publisher
Rodgers, J., 2012. Anti-oppressive social work research: Reflections on power in the creation of knowledge. Social Work Education, 31(7): 866-879.View at Google Scholar | View at Publisher
Saldana, J., 2014. The coding manual for qualitative researchers. 2nd Edn., London, UK: Sage Publications.
Scott, J., D. Varghese and J. McGrath, 2010. As the twig is bent, the tree inclines: Adult mental health consequences of childhood adversity. Archives of General Psychiatry, 67(2): 111-112. View at Google Scholar | View at Publisher
Siegel, J.D., 2012. The developing mind: How relationships and the brain interact to shape who we are. New York: The Gilford Press.
Strier, R., 2006. Anti-oppressive research in social work a preliminary definition. British Journal of Social Work, 40(6): 1908–1926.View at Google Scholar | View at Publisher
Szalavitz, M. and B. Perry, 2010. Born for love: Why empathy is essential and endangered. New York: Harper Collins Publishers.
Taylor, S., 2015. The trauma-informed classroom training guide. Phnom Penh, Cambodia: Hagar International.
Thorne, S., 2010. Applied interpretation: A Review of interpretive description by Sally Thorne. Qualitative Report, 15(6): 1624-1628. View at Google Scholar
Thorne, S., S. Kirkham and J. MacDonald-Emes, 1997. Interpretive description: A noncategorical qualitative alternative for developing nursing knowledge. Research in Nursing, 20(2): 169-177.View at Google Scholar | View at Publisher
Thorne, S., S. Kirkham and K. O’Flynn-Magee, 2004. The analytic challenge in interpretive description. International Journal of Qualitative Methods, 3(1): 1-22.View at Google Scholar | View at Publisher
Walkley, M. and T.L. Cox, 2013. Building trauma-informed schools and communities. Children & Schools, 35(2): 123-126.
Westoby, P. and A. Ingmells, 2010. A critically informed perspective of working with resettling refugee groups in Australia. British Journal of Social Work, 40: 1759-1776. View at Publisher
Wyatt, Z., E. Hoban, S. Macfarlane and M. Nowlin, 2017. Being trauma-informed in Cambodia: practice considerations for professionals working with children and trauma. International Journal of Social Science and Humanity, 7(6): 442-448.
Wyatt, Z. and L. Oliver, 2016. Y-change: Young people as experts and collaborators. Advances in Social Work and Welfare Education, 18(1): 121-126. View at Google Scholar
Zeigler, D., 2013. Optimum learning environments for traumatized children: How abused children learn best in school. Jasper Mountain: 1-8. Retrieved from http://www.jaspermountain.org/.