




THE PERCEPTIONS OF MOTHERS ON THE USE OF NON- SKILLED MATERNAL HEALTHCARE IN KENYA

1Great Lakes University of Kisumu and The Delta Centre, Kitengela, Kenya, 2Great Lakes University of Kisumu, Nairobi Learning Centre, Kenya , 3International United Nations Volunteer Midwife, UNFPA, Wau, Western Bahr El Ghazal State, Republic of South Sudan
ABSTRACT
Forty three percent (43%) of deliveries in Kenya takes place under the supervision of skilled attendants. But the Nyanza province in Western Kenya still registers lower proportions of facility deliveries (34 percent). But in Siaya district of the Nyanza province, only 30 percent of mothers utilize skilled maternal health care. A sequential exploratory mixed study was conducted in Uranga, North Alego and Karemo divisions of Siaya district and interviewed 1197 mothers who had home deliveries a year prior to the study. Another 11 key informants were interviewed comprising community specialists in the Luo traditional maternal healthcare medicine, skilled health workers serving in the facilities located in each of the three divisions; traditional Luo medicine men and women; and religious maternal health care providers who also doubled as spiritual overseers within their divisions. The objective of the study was to establish the perceptions of mothers on the use of non-skilled maternal healthcare. The study established the frequencies and the effect size of the selected variables whose relationships were measured and indicated by the p value of the Wald statistics in a multinomial regression model. The Wald chi-square p value <0.05 indicated significant results while qualitative data was manually analyzed by condensing and organizing responses in meta cards, teasing them out into common themes and then clustering them in tandem with the objective of the study. Each cluster was partitioned and coded (from a code list, which the researcher and the team developed) then the emerging phrases were summarized, compressed and assembled to draw conclusions and recommendations. The study found that as long as the skilled maternal healthcare system remain ineffective in providing accepted remedies related to correcting and reversing taboos, abominations, curses and healing the spiritual being of the mothers, then the mothers will continue utilizing the non skilled maternal care.
© 2017 AESS Publications. All Rights Reserved.
Keywords: Perception, Non skilled maternal healthcare, Kenya. Skilled maternal healthcare, Luo traditional maternal healthcare, Mothers, Taboos, Abominations, Curses, Treatment regimes
Received: 13 April 2016/ Revised: 4 May 2016/ Accepted: 24 August 2016/ Published: 28 November 2016
Contribution/ Originality
This study is one of very few studies which have investigated the opinions of mothers on the use of non-skilled maternal health care. Most papers have focused on the use of skilled attendants and have not effectively interrogated the opinions of women on why they specifically use non-skilled care.
1. INTRODUCTION
Kenya is among the Sub-Saharan African countries that still has a large proportion of its population carrying the highest burden of ill-health (Ministry of Health, 2006; Kaseje et al., 2009). This includes maternal mortality rate of 590 deaths per 100,000 live births in 1998 (Ministry of Planning and National Development, 2005) down to 414 deaths per 100,000 live births in 2002 (Ministry of Public Health and Sanitation, 2009) up to 488 deaths per 100,000 live births (Kenya Demographic and Health Survey Report, 2010).
KDHSR (2010) indicate that less than 47 percent of pregnant women make four antenatal visits. For instance, 60 percent of pregnant women in urban areas make four antenatal visits compared to 44 percent in the rural areas. Only 15 percent obtain the four antenatal visits as recommended. Regional disparities are noted in antenatal coverage. While mothers in North Eastern province do not get antenatal care at all, Nyanza and Western provinces have low use of doctors for antenatal care compared with use of nurses, with Coast and Central provinces registering the reverse (Ibid, 115).
In the same report (Ibid: 120), it is indicated that 43% of deliveries in Kenya take place under the supervision of skilled attendants. This is indicative of a 3% increase since the year 2003 which registered 40%. However, provinces such as Nyanza in western Kenya still register lower proportions of facility deliveries (34 percent). However, the Tropical Institute of Community Health and Development in Africa and Kaseje et al. (2009) found that less than one third (30 percent) of mothers use health facility delivery in Siaya district in Nyanza province. Overall, the distribution of mothers that do not deliver under skilled supervision remain high in a number of provinces including North-Eastern (81 percent), Western (73 percent), Rift Valley (66 percent) and Nyanza (54.9 percent). Regarding the use of postnatal care ibid indicates that 37 percent of women receive postnatal care from medical professionals, with Nairobi having the largest proportion of mothers (78 percent) accessing postnatal care. The objective of the study was to examine the perception of mothers on the use of non-skilled maternal healthcare.
2. RESEARCH METHODOLOGY
The study employed a sequential exploratory mixed study design. Four methods of sampling were used. These were; multistage cluster sampling, purposive, stratified, and random sampling. A total of 1197 mothers who had home deliveries a year prior to the study were sampled in Uranga, North Alego and Karemo divisions of Siaya district. Another 11 key informants were interviewed comprising community specialists in the Luo traditional maternal healthcare medicine, skilled health workers serving in the facilities located in each of the three divisions; traditional Luo medicine men and religious maternal health care providers who also doubled as spiritual overseers within their divisions. The study was conducted in three phases. The first was the listening survey to establish the generative themes on the perceptions between the skilled and non-skilled maternal healthcare systems; the second was the collection of qualitative data derived from the generative themes; and the third and final was the collection of quantitative data whose themes and variable were derived from the qualitative data that were analyzed.
Frequencies and effect size of the selected indicators whose relationships were measured and indicated by the p value of the Wald statistics in a multinomial regression model were established. The Wald chi-square p value <0.05 indicated significant results. Qualitative data was manually analyzed where data was condensed by organizing responses in meta cards, then teasing them out into common themes and then clustering them in tandem with the objective of the study. Each cluster was partitioned and coded (from a code list, which the researcher and the team developed) then the emerging phrases were summarized. These were further compressed and assembled to draw conclusions and recommendations.
3. RESEARCH RESULTS
The study interviewed 1197 respondents drawn from Karemo (392), Uranga (424) and Boro (381) divisions in Siaya District. The respondents were mothers who had their last deliveries at home a year prior to this study. The highest proportion (39%) were between 21-29 years while 50 % had between 1-3 children with 2 percent having more than 10 children. Although the highest percentage (30%) who delivered at home ascribed to the African religious churches, Roman Catholic followers (29 %), Anglican and Pentecostal churches (19%) respectively were equally present.
Table-1. Characteristics of respondents
| Variables | N | Percentage |
| Division | ||
| Karemo | 392 | 32.9 |
| Uranga | 424 | 35.4 |
| Boro | 381 | 31.8 |
| Age | ||
| 15-20 | 279 | 23.3 |
| 21-29 | 467 | 39.0 |
| 31-39 | 332 | 27.7 |
| 40-49 | 114 | 9.5 |
| Missing | 5 | 0.4 |
| No. of Children | ||
| 1-3 | 592 | 49.5 |
| 4-6 | 414 | 34.6 |
| 7-10 | 155 | 12.9 |
| Above 10 | 21 | 1.8 |
| Missing | 15 | 1.3 |
| Denomination | ||
| Catholic | 348 | 29.1 |
| Anglican | 221 | 18.5 |
| Pentecost | 231 | 19.3 |
| AfricanTraditionalChurch | 355 | 29.7 |
| Missing | 42 | 3.5 |
N=11
3.1. The Care Providers in the Non Skilled Maternal Healthcare System
The study found an array of groups that provided the most care to mothers during the last pregnancy. These were community health workers (39%), traditional birth attendants (29%), churches (14%) and relatives (11%). When these providers were asked why they offered care in the non skilled maternal healthcare system against the policy of the Ministry of Health, they explained that the policy was not privy to the strengths of the traditional maternal healthcare system which they also referred to as the non-skilled maternal healthcare. However, they offered the care in secrecy to avoid reprimand by the authorities.
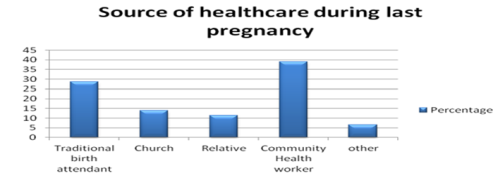
Figure-1. Where did you get the most care during your last pregnancy?
N=1197
On the other hand, community health workers (48%) provided the most care to mothers during the last delivery followed by traditional birth attendants (24 %), churches (12%) and relatives (10%). The study found that the community health workers referred to here had both conventional skills in preventive health as well as traditional maternal healthcare skills that they often put to use when delivering pregnant women. However, the traditional birth attendants referred to here had no form of training except those passed on to them by their parents and grandparents.
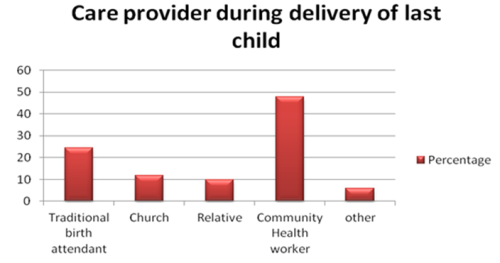
Figure-2. Who provided you with care during the delivery of your last child?
N=1197
The study found that 83 percent (995) of mothers were aware of the benefits of using skilled prenatal care during pregnancy; 77 percent (917) knew the benefits of facility delivery and 86 percent (1023) were knowledgeable of the benefits of attending skilled postnatal care respectively. However, none of them delivered at the health facilities. This was because 722 (60 percent) of respondents had herbs for shortening the duration of labour within their communities. Of these, 28 percent used the herbs to shorten labour during the last pregnancy in addition to 773 (64.6 percent) who reported the existence of traditions (Chike Luo) that they were expected to follow during the last pregnancy, but which were not available in the health facilities.
Presence of traditional methods used for providing care to women in the first three months after delivery was also reported by 832 (70%) of respondents of which 614 (51 %) had used the methods after the last delivery. Another 410 (34 %) used traditional methods of child spacing after the birth of the last child. A significant relationship between the presence of herbs used to shorten the duration of labour by where the mother received the most care during the last pregnancy (p value= .001) was found. Subsequently, the study also reveals a significant relationship between the use of the traditional herbs for shortening the duration of labour and where the mother received the most care during the last pregnancy (p value=.000). However, there is no significant relationship between the presence of traditions (Chike Luo) that communities expect a new born baby to undergo; the presence of traditional methods used for child spacing after the birth of the last child by where the mother received the most care as both have a P value of 0.111 and .007 respectively.
Table-2. Percentage proportion of selected indicators on perceptions on non-skilled maternal healthcare
| Factors | n | Percentage | |
| Are there herbs used in your community to shorten the duration of labour | Yes | 722 | 60.0 |
| No | 294 | 24.6 | |
| Missing | 181 | 15.2 | |
| If yes, did you use these herbs to shorten the duration of labour during your last pregnancy? | Yes | 338 | 28.2 |
| No | 566 | 47.3 | |
| N/A | 245 | 20.5 | |
| Missing | 48 | 4.0 | |
| Are there traditions (Chike Luo) that your community expects a new baby to undergo? | Yes | 773 | 64.6 |
| No | 410 | 34.3 | |
| Missing | 14 | 1.2 | |
| Are there traditional methods you used for child spacing after the birth of your last child? | Yes | 426 | 35.6 |
| No | 764 | 63.8 | |
| Missing | 7 | 0.6 | |
| Are there traditional methods that are used to provide care to a woman in the first three months after delivery? | Yes | 832 | 69.5 |
| No | 341 | 28.5 | |
| Missing | 24 | 2.0 | |
| If yes, did you ever use these traditional methods after the birth of your last child? | Yes | 614 | 51.3 |
| No | 494 | 41.3 | |
| Missing | 89 | 7.4 |
Source: Primary interviews
3.2. Pregnancy Management in the Non-Skilled Maternal Healthcare System
The non-skilled maternal healthcare system has remedies for managing complications during pregnancy in addition to the provision of traditionally acceptable meals to the expectant mother during the pre-natal visits. Although Okolocha et al. (1998) and Griffin (2006) had similar findings in Southern Nigeria and India respectively, meals served to pregnant mothers during their regular visits by the traditional maternal healthcare providers did not suffice as in the case of this study. These preferences are only found in the non-skilled maternal healthcare systems, a finding that supports (Annette, 2004).
Other aspects include the ability of the care givers to communicate with the spirits to determine the spiritual health of the pregnancy, provision of remedies in cases where pregnant woman suffers from spiritual related conditions, sponging of pregnant women with hot water to provide comfort and management of pregnant related ailments. These aspects endeared mothers more to the non-skilled maternal healthcare as compared to facility based care.
The hospitality of the healthcare providers in the non skilled system was commended by women for they do not quarrel with pregnant women as they attend to them during labour. Mothers mentioned the absence of caesarian section in the non-skilled maternal healthcare system which makes them comfortable to seek for care. They also noted that non-skilled maternal healthcare providers do not continuously insert their hands in the vagina of pregnant women who are in labour. The ability of the non-skilled maternal healthcare providers to determine when the unborn baby is in danger by simply touching the abdomen of the pregnant woman, privacy and asking her questions regarding her comfortability were reported by the respondents as having endeared mothers to the non-skilled maternal healthcare. Aspects such as privacy during delivery and language of communication that Annette (2004) brought to the fore were not the case in this study. The foregoing therefore challenges the skilled maternal healthcare system that as long as these preferences are not observed, then women will continue to utilize non-skilled maternal healthcare system.
Table-3. Treatment regimes during pregnancy
| S/N | Type of treatment | Purpose | Description of administration |
| 1. | Ochwaga | Administered to women who suffer from swollen legs to accompany | Boiled, then the mother drinks the mixture |
| 2. | A mixture of water, lemon, menthol sweets, and ginger, depack cream, coca cola soda, green candle and garlic onions | Given to all pregnant women, which also reverses the curses or problems related to attacks by evil spirits (Juogi) | First taken in the presence of the providers then the rest is stored in a bottle or any container to be taken twice for three days. |
| 3. | Depack cream1 used to massage the mother upwards and downwards around the stomach and back up to the location of the umbical | Helps to ease bowel movement and relaxation of muscles | Administered from the fourth month of pregnancy till delivery and after delivery |
| 4. | Rabongo | TrearaOPPED HERE on inl health caret natal care. fixed included and attitudes g prenatal care clini, facility deliverya e is .000 its swelling and body pains in pregnant women. It helps expectant mother to pass urine – a process that helps to clean the kidney. The drink also enables the fetus to move about | Boiled and taken on daily basis |
| 5. | Yath Koko/koke | Treats koko – an infections as a result of a pregnant mother consuming meat from an animal that has been killed by a hyena (Ondiek). | Boiled and taken on daily basis |
| 6. | Kuogo | Treats Sexually Transmitted Infections in pregnant mothers | Mixed Ober and boiled then taken daily while some are mixed with water and used for bathing. |
| 7. | Ober | Treats koko – an infections as a result of a pregnant mother consuming meat from an animal that has been killed by Ondiek (hyena) | Mixed with Kuogo then taken orally and also used for bathing. |
| 8. | Yath Chira/ Yiend Chiche | Administered to a woman who is having a miscarriage. Administered by a special persons called Ja Yath Chira | They boil, drink and bath in it |
| 9. | Okwer Gw’eno | Treats a condition known as ‘Orianyanja’ in infants, it also treats fungal infections in the private parts of expectant mothers and infants | It is boiled and administered to children/ mothers three times a day |
| 10. | Olan’g langwe | Treats swelling (bunda) during pregnancy and infections in new borns | Boiled then the mother and baby bath with it |
| 11. | Abar Dakuon | Treats scabies in pregnant women and new born babies | The mixture is applied on the affected skin |
| 12. | Tiend Oyieko | Used for treating skin ulcers in mothers during and after pregnancy | Boiled and drunk and used for bathing by the mother |
| 13. | Nyatiend Gw’eno | Used for treating boils in pregnant women and infants | The leaves are smashed, then wrapped on another leaf, then it is mixed with cob wed and tied on the boil. |
| 14. | Yath Marate’ng | Used during pregnancy to massage the stomach so that a breech baby can turn to the desired position | Massage is done using upward and downwards movement using the 4 fingers and at times releasing the thumb to massage the lower abdomen. |
| 15. | Ogal | Administered to women during pregnancy to clean the reproductive system | Boiled then mixed with porridge and served to a pregnant woman |
Source: Primary interviews with spiritual traditional maternal healthcare providers
3.3. Management of Deliveries in the Non Skilled Maternal Healthcare System
In the non-skilled maternal healthcare system, deliveries are managed with the comfort of the laboring woman in mind. This is done by ensuring that before delivery, the body of the woman is sponged using warm water and her preferred position of delivery is established and respected. To this end, squatting and kneeling positions were mainly preferred during delivery. The care provider then supports the woman to pace up and down the homestead to allow the baby to move towards the cervix, a process which stops as soon the woman begins to feel the baby’s head moving towards the vagina. The study further found that management of complications related to delivery are in many ways dependent on the nature of complication. For instance, in the event that there was delay in delivery of the baby or the placenta, the woman was asked to kneel down to allow the baby to move towards the vagina. While in the kneeling position, the woman is asked to open her mouth and a wooden cooking spoon (Oliho) or rosary, is placed in her throat. This is done to choke her so as to trigger vomiting. As she attempts to vomit, pressure is mounted from her stomach that pushes the baby or the placenta out.
They noted that although the health facilities view the placenta as a mere after birth, its disposal in the traditional realm determines whether or not the mother will conceive in the future. When asked why this was the case, respondents explained that there was a specific way that a placenta has to be disposed of. This involves rolling the placenta slowly in a hole while holding the tip of the umbilical code that was cut and when the entire placenta settles in the hole, the provider ensures that the tip remains in an upwards position. This signifies an open doorway to future pregnancies by the mother that has just delivered. If the tip is buried facing downwards then the mother will never conceive and /or give birth again. The placenta is also buried behind the house of the woman that has just delivered. Traditions do not allow one to cross over to the other side of the homestead (Nga’do dipo) to bury the placenta; such an action leads to inability of the woman to deliver other babies.
Reports from the mothers interviewed also indicated that the non-skillsed maternal healthcare providers do not stitch mothers to ensure that the perenial tears heal properly and the perineum returns to its normal shape after delivery. They said that the providers sponge mothers who have had perennial tears during child birth using hot water and salt, and during this process, the woman is asked to contract and relax at regular intervals the muscles around the vagina as though she is withholding and passing urine. Respondents explained that this process enables the muscles around the vagina to get toned back to the pre delivery state.
The absence of male care givers in the non-skilled maternal healthcare was noted by the respondents as having made the services free from sexual abuse. When mothers were asked to explain how they encountered sexual abuse in health facilities, they explained that male health care workers sometimes touched women’s external sexual organs without any professional justification. This case was strongly cited by mothers at Malanga and Nyajuok. The mothers said that such incidences do not happen under the care of the non-skilled maternal healthcare providers.
3.4. Post-Natal Care in the Non-Skilled Maternal Healthcare
Post-natal care was described by respondents to include feeding and care of mothers after delivery, removal of placenta in cases of retention, treatment of conditions that affect mothers after delivery and methods of child spacing. Regarding the feeding given to mothers after delivery, mothers reported that care givers in the non-skilled health system provide them with black tea mixed with lemon to help in removing the blood clots. In addition, they [mothers] are also massaged using a herb known as manyasi to force the placenta out in the event that the placenta is not expelled within the normal duration.
Besides the massaging to help the mothers to push out the placenta, it also helps the mother with bowel movement as well as treats a condition called Arip which occurs when the birth canal is blocked. When asked to describe Arip, the respondents said that the pain associated with Arip is felt around the vagina and is also characterized with needle-like pricking pain. Another condition described by respondents which was addressed through massage was Bunda (swelling of the body), which they said makes delivery difficult because a pregnant woman may not be able to push the baby during labour due to increase in weight as a result of the swelling.
The ability of the non-skilled maternal healthcare system to prevent pregnancy was reported by mothers as one of the methods that contributed to their satisfaction with the non-skilled system. Among these methods include Tweyo, a method which was reported as having no side effects on mothers because it involves taking the under wear of a women who has just delivered , then tying it with a piece of placenta. ems. The two tied items are placed over the traditional cooking place called Oyare to prevent the woman from conceiving. This procedure is known as Ngawo dhako (blocking the womb of a woman from conception) But when the woman is ready to conceive another baby, the item is removed from Oyare by the same traditional maternal healthcare provider who had performed the initial procedure. This act of removing the item from Oyare is a sign that the woman’s womb is ready to carry another pregnancy.
Other than the rituals mentioned above related to birth control, respondents mentioned a number of taboos that equally hinder pregnancy from taking place. These are associated with the cultural sanctions put in place to safeguard the planting and harvesting seasons; mourning period and the norms that couples are expected to observe during this period. During the planting season known as Chwiri, members of a homestead are not allowed to go to the farm and plant the first seeds ahead of the head of the homestead. The head of a homestead in this case is the man whose house stands directly facing the main gate (Rang’ach) of the home. Respondents said that the Luo community has a clear distinction between the main gate and Roth (an opening around the fence of the homestead). A night before the first planting day, the head of the homestead is expected to have sex with his wife as a sign of successful planting. This ritual is called Golo Kodhi. Any woman who goes ahead to have sex with her spouse who is not a homestead head cannot conceive. The same pattern is followed during the harvesting period. Additional taboos that women associated with blockage of conception included having sexual intercourse when a co-wife to a mother- in- law has died. The women noted that during the mourning period, every sexually active person in the homestead refrains from sexual intercourse for a period of one week, and that should this sanction be broken, then no pregnancy can occur. Finally, respondents reported that when a woman has delivered, the husband is not allowed to come closer to her because she still smells blood as a result of child birth (also called Nyaudo or Nyawiwo in Dholuo Language). For this reason, sexual relationship between women who have delivered and their husbands are less likely to occur. Although unborn babies and pregnant women suffered from conditions that could only be managed within the skilled maternal health care system, the key informants interviewed at the health facilities in Nyoderea, Kaluo and Siaya district hospital observed that the dialogue between the traditional and skilled maternal healthcare systems has remained weak.
Table-4. Treatment regims during delivery
| S/N | Type of treatment | Purpose | Period of administration |
| 1. | Yath Chira/ Yiend Chiche | Administered to a woman who is having a miscarriage. Administered by a special persons called Ja Yath Chira | They boil, drink and bath in it |
| 2. | Nyatik Oten’ga | Used to shorten labour | Is burnt on fire then chewed by mother during labour |
| 3. | Tiend Orian’g | Used to shorten labour in cases where traditional maternal healthcare providers establish that labour is prolonged | The roots are burnt on fire, then chewed by the mother |
| 4. | Tiend Oyieko | Used for treating skin ulcers in mothers during and after pregnancy | Boiled and drunk and used for bathing by the mother |
| 5. | Yath Winyo | Administered to infants who are born before full term 7- 8 months and beyond | Drops of the mixture are given to the infant through the mouth |
| 6. | Nyalwet kwach | Administered after delivery to ease back pain, stomach ache and general pains that occur after delivery | Boiled and drunk by women |
| 7. | Pado | Used to lower blood pressure after delivery and relieving of body pain | Boiled and drunk by a mother who complains of dizziness, energy loss as this is regarded as a sign of high blood pressure. |
Source: Primary interviews
Table-5. Relationship between perceptions on non-skilled maternal healthcare systems and where the mother received the most care during the last pregnancy
| Variables | Wald Chisquare p value |
| 1. Are there herbs in your community used to shorten the duration of labour for women by where did you receive the most care during your last pregnancy | 0.001 |
| 2. Did you use these herbs to shorten the duration of labour during your last pregnancy by where did you receive the most care during your last pregnanc | 0.000 |
| 3. Are there traditions (Chike Luo) that your community expects a new born baby to undergo by where did you receive the most care during your last pregnancy | 0.111 |
| 4.Are there traditional methods you used for child spacing after the birth of your last child by where did you receive the most care during your last pregnancy | 0.007 |
| 5. Are there traditional methods that are used to provide care to a woman in first three months after delivery by where did you receive the most care during your last pregnancy | 0.000 |
| 6. Are there traditional methods that are used to provide care to a woman in first three months after delivery by where did you receive the most care during your last pregnancy | 0.000 |
| 7. Are there taboos that restricted you from having sexual relationship with their partner after the birth of your last child by where did you receive the most care during your last pregnancy | 0.024 |
| 8. If yes, did you follow these taboos after the birth of your last child by where did you receive the most care during your last pregnancy | 0.001 |
| 9. Are there any form of taboos (Kweche) that restrict you from sexual intercourse with their partners at any given time of their life by where did you receive the most care during your last pregnancy | 0.004 |
| 10. Are there practices in your household which enabled you to space your children without necessarily using family planning methods or herbs by where did you receive the most care during your last pregnancy | 0.945 |
N=1197
4. CONCLUSION
The study has found a significant relationship between the presence of herbs used to shorten the duration of labor and where a mother received the most care during the last pregnancy (p value= 0.001); and between the use of the traditional herbs for shortening the duration of labor and where the mother received the most care during the last pregnancy (p value=0.000). Also revealed is the absence of relationship between the presence of traditions (Chike Luo) that communities expect a new born to undergo; the presence of traditional methods used for child spacing after the birth of the last child by where the mother received the most care during the last pregnancy as both have a p value of 0.111 and .007 respectively. The finding of this study suggests that the management of pregnancy using non-skilled maternal healthcare is viewed as superior because of various reasons including; ability to correct / reverse the taboos, abominations and curses; healing the spiritual part of the mother by providing prayers; administering concoctions to women and their spouses, massaging of pregnant women and ability to listen to the voices of the spirits in relation to the instructions given on a iven pregnancy, delivery and post natal care. The African traditional churches grant the traditional maternal healthcare service providers authority to deliver babies, but the ministry of health policy does not. This has created a contradiction because the traditional maternal healthcare system which is viewed by the African traditional churches as being capable of managing conditions that are beyond the capacity of the skilled maternal healthcare system but which is not granted permission. This study suggests that the non-skilled maternal healthcare is not only preferred during pregnancy and labour, but also during delivery. Among the aspects that make delivery in the non-skilled maternal healthcare more preferred included the sponging of pregnant women who are in labour with warm water; being supported to pace up and down the homestead to help with movement of the baby towards the cervix; remedies used to address complications during delivery such as prolonged labour and delay in the delivery of the placenta. Overall, the knowledge on the benefits of utilizing skilled maternal healthcare during pregnancy, delivery and post natal care is not sufficient to inspire women to seek skilled maternal healthcare. As long as the skilled maternal healthcare system remains ineffective in providing accepted remedies related to correcting and reversing taboos, abominations, curses and healing the spiritual being of the women , then women will continue utilizing the traditional system. Other critical offerings in the traditional systems include provision of prayers and communicating to the spirits and adhering to the directives, massaging mothers and managing labor and delivery in more natural ways.
5. RECOMMENDATIONS
It is evident from the findings of this study that the skilled maternal healthcare system cannot ignore the strengths of the non skilled maternal healthcare system. This is deduced from the premise that the skilled maternal health system cannot handle the maternal healthcare complications related to spirits, curses and abominations. ve .this prevailing perceptions require that the skilled and non-skilled maternal healthcare systems. dialogue to establish areas of interface. Key to this dialogue is how the skilled maternal healthcare system can work closely with the non skilled maternal healthcare system to address maternal health conditions related to spirituality, treatment of ancestral curses and abominations and other non biometric conditions that are better understood in the traditional maternal healthcare realm.
| Funding: This study received no specific financial support. |
| Competing Interests: The authors declare that they have no competing interests. |
| Contributors/Acknowledgement: All authors contributed equally to the conception and design of the study. |
REFERENCES
Annette, N., 2004. Factors influencing utilization of postnatal services in Mulago and Mengo Hospitals, Kampala, Uganda: A Mini Thesis Submitted in Partial Fulfillment of the Requirements for the Degree of Master of Science in Physiotherapy in the Department of Physiotherapy, University of Western Cape.
Griffin, S., 2006. Literature review on sexual and reproductive health rights: Universal access to services, focusing on east and Southern Africa and South Asia. London: Realizing Rights.
Kaseje, D., R. Olayo, C. Musita, C. Oindo, C. Wafula and R. Muga, 2009. Evidence based dialogue with communities for district health systems performance improvement. Global Public Health, 00(0): 1-16.
Kenya Demographic and Health Survey Report, 2010. Nairobi: Kenya Bureau of Statistics.
Ministry of Health, 2006. Reversing the trends: The second national health sector strategic plan of Kenya: Taking the Essential Package for Health to the COMMUNITY: A Strategy for the Delivery of LEVEL ONE SERVICES, Health Sector Reform Secretariat. Nairobi.
Ministry of Planning and National Development, 2005. Courtesy of UNDP Kenya and the Government of Finland. Millennium Development Goals in Kenya: Needs and Costs.
Ministry of Public Health and Sanitation, 2009. National road map for accelerating the attainment of MDG’s related to maternal and newborn health in Kenya. Nairobi. Available from http://www.health.go.ke.
Okolocha, C., J. Chiwuzie, S. Braimoh, J. Unuigbe and P. Olumeko, 1998. Socio-cultural factors in maternal morbidity and mortality: A study of semi urban community in Southern Nigeria. Epidemiol Community Health, 52(5): 293-297.
BIBLIOGRAPHY
African Union Commission, 2008. African union commission: Assessing progress in Africa towards the Millennium development goals report: A Joint Annual Meeting of the African Union Conference Ministers of Economy and Finance and ECA Conference on African Ministers of Finance, Planning and Economic Development: Forty First Session of the Economic Commission for Africa in Addis Ababa.
Chibwana, A.I., D.P. Mathanga, J. Chinkhumba and C.H. Campbell, 2009. Socio-cultural predictors of health seeking behaviour for febrile under five children in Mwanza, Neno district, Malawi. Malaria Journal, 8: 219.
Eyayou, Y., 2003. Socio-cultural factors in decisions related to fertility in remotely located communities: The case of Suri ethnic group: A Thesis Submitted to the School of Graduate Studies of Addis Ababa University in Partial Fulfillment of the Requirements for the Degree of Masters of Public Health, Department of Medicine, Addis Ababa University.
Family Health International, 2006. Behavioral change – a summary of four major theories. Behavioural Research Unit. Available from http://www.fhi.org.
Fotso, J.C., A.C. Ezeh and H. Essendi, 2009. Maternal health in resource poor urban settings: How do women’s autonomy influence the utilization of obstetric care services. Reproductive Health Journal, 6(9): 1-8. DOI 10.1186 /1742-4755-6-9.
Freire, P., 1998. Education for critical consciousness. New York: The Continuum Publishing Company.
Furuta, M. and S. Salway, 2006. Women’s position within the households a determinant of maternal health care us in Nepal. International Family Planning Perspective, 32(1): 17-27.
Grady, K.E. and B.S. Wallston, 1988. Research in health care settings. London: Sage Publications.
Gule, G., 1994. Socio-cultural constraints to family planning in Swaziland. Canadian Studies in Population, 21(1): 55-59.
Hardon, A., P. Boonmongkon, P. Streetfland, M.L. Tan, T. Hongvivatana, D.G.S. Van , S.A. Van , C. Varkevisser, L. Acuin, M. Chowdhury, A. Bhuiya, L. Stringeryuang, E. Van Dongen and T. Gerrits, 2001. Applied health research: Anthropology of health and health care. Amsterdam: Het Spinhuis Publishers.
Hope, A. and S. Timmel, 1995. Training for transformation: A handbook for community workers- book 1. Nottingham: Intermediate Technology Publications.
Hruschka, D.J. and C. Hadley, 2008. A glossary of culture in epidemiology. J Epidemiol Community Health, 62(11): 947-951.
Jegede, A.S., A.S. Ajala, O.P. Adejumo and S.O. Osunwole, 2006. Forced feeding practice in Yoruba community of Southern Western Nigeria: Evidence from ethnographic research. Anthropologists, 8(3): 171-179.
Kinney, V.M., J.K. Kerber, E.R. Black, B. Cohen, F. Nkrumah, H. Coovadia, M.P. Nampala and J. Lawn, 2010. Sub Saharan Africa’s mothers, newborns and children, where and why do they die? On behalf of the science in action: Saving the lives of Africa’s mothers, newborns and children working group. Available from /10.137/journal.pmed.1000294.
Lawoyin, O.T., L.O. Lawoyin and D. Adewole, 2007. Perception of maternal mortality in Nigeria. Journal of Public Health Policy, 28(3): 299-318.
Leedy, P.D. and J.E. Ormrod, 2005. Practical research: Planning and design. 8th Edn., Columbus: Pearson Mewill Prentice Hill.
Lhamu, C., 2004. Factors effecting utilization of contraceptives among married women of reproductive age (15-49) years in Punakha district, Bhutan. A Thesis Submitted in Partial Fulfillment of Requirements for the Degree of Masters of Public Health in Health Systems Development, College of Public Health, Chulalongkorn University.
Lubbock, A.L. and B.R. Stephenson, 2008. Utilization of maternal health care services in the department of Matagalpa, Nicaragua. Rev Panam Salud Publica /Pan Am/Public Health, 24(2): 75-84.
Magadi, M., 2006. Poor pregnancy outcomes among adolescents in South Nyanza region of Kenya. African Journal of Reproductive Health, 10(1): 26-38.
Miles, M.B. and A.M. Huberman, 1994. An expanded source book: Qualitative data analysis. 2nd Edn., London: Sage Publications.
Ministry of Finance and Planning, 2001. Siaya district development plan: 2002-2008: Effective management for sustainable economic growth and poverty reduction. Nairobi: Government Printers.
Moronkola, O.A., M.M. Ojediran and A. Amosu, 2006. Reproductive health knowledge, belief and determinants of contraceptive use among women attending family planning clinics in Ibadan, Nigeria. Afri Health Science, 6(3): 155-159.
Mothibeli, M.L., 2009. Factors influencing utilization of VCT and testing of HIV among pregnant women of Lesotho. A Dissertation Submitted in Partial Fulfillment of the Requirements for the Master in Population Studies in the Graduate Programme in the Faculty of Humanities Development and Social Sciences, University of KwaZulu Natal, Durban.
Mugenda, O. and A. Mugenda, 2003. Research methods; qualitative and quantitative approaches. Nairobi: Acts Press.
Munro, S., S. Lewin, T. Swart and J. Volumink, 2007. A review of health behaviuors theories: how useful are these for developing interventions to promote long-term medication adherence for TB and HIV / AIDS. BMC Public Health, 7(1): 104. DOI 10.1186/1471-2458-7-104.
National Cancer Institute, 2005. U.S department of health and human services, and national institute for health. 2nd Edn. Theory at a Glance: A Guide for Health Promotion Practice: NIH Publication No. 05-3896
Ng’ombe, J. and Kasiya, 2006. The extent of inequalities in relation to maternal and new born health at community level: A baseline study in Ntchisi district, Malawi. Malawi Medical Journal, 18(2): 72-76.
Obure, M.J., 2002. Handbook on data analysis using SPSS version 10.0: Learning and using SPSS for windows is made simpler and easier. Nairobi: M & O Data Experts Training and Consultants.
Oindo, C.O., C.F. Otieno, N.O. Okeyo, R.N. Olayo, R.O. Muga and C.O. Kaseje, 2009. Characteristics of households experiencing under 5 deaths: A case study of the tropical institute of community health and development (TICH) partnership districts. African Journal of Food, Agriculture, Nutrition and Development, 9(3). DOI http://dx.doi.org/10.4314/ajfand.v9i3.43013.
Omondi, D.O., M.K. Walingo, G.M. Mbagaya and L.O.A. Othuon, 2010 Advancing the theory of planned behaviour within dietary and physical domains among type 2 diabetics: A mixed methods approach. World Academy of Science, Engineering and Technology: International Journal of Social, Behavioural, Educational, Economic, Business and Industrial Engineering, 2(3): 1599-1606.
Opiyo, P., T. Yamano and T.S. Jayne, 2008. HIV /AIDS and home based health care. International Journal for Equity in Health - The official Journal of the International Society for Equity in Health, BioMed Central Ltd, 7(8). DOI 101186/1475-9276-7-8.
Oxaal, Z. and S. Cook, 1998. Health and poverty gender analysis: Briefing prepared for the Swedish international development cooperation. BRIDGE Development, Gender Report, No. 46, Institute of Development Studies, University of Sussex.
Ranson, I.E. and V.N. Yinger, 2002. Making motherhood safer: Overcoming obstacles on the pathway to care, Population Reference Bureau, Washington D.C. Available from http://www.prb.org/.
Rao, P.V., 1998. Statistical research methods in life science. Washington: Duxbury Press.
Saleemi, N.A., 1997. Quantitative techniques simplified: A text book for quantitative techniques papers of CPA, CICT and other examining bodies. Nairobi: ACME Press.
Say, L. and R.A. Raine, 2007. A systematic review on inequalities in the use of maternal health care in developing countries: Examining the scale of the problem and the importance of context. WHO Bulletin, 85(10): 733-820.
Sim, J. and C. Wright, 2000. Research in health care: Concepts, designs and methods. Cheltenham: Stanley Thomas Publishers.
Simkhada, B., A.M. Porter and V.R.E. Teijingen, 2001. Role of mothers-in-law in antenatal care decision making in Nepal: A qualitative study. BMC Pregnancy Childbirth, 10(34). DOI 10.1186/1471-2393-10-34.
Stephenson, R., A. Bashchieri, S. Clements, M. Hennink and N. Madise, 2007. Contextual influence on modern contraceptive use in Sub Saharan Africa. American Journal of Public Health, 97(7): 1233–1240. DOI 10.2105/AJPH-2005.071522.
Thairu, L.N., H.G. Pelto, C.N. Rollins, M.R. Bland and N. Ntshangage, 2005. Socio-cultural influence on infant feeding decisions among HIV-infected women in rural KwaZulu Natal, South Africa, Blackwell Publishing Ltd. Maternal and Child Nutrition, 1(1): 2-10. DOI 10.1111/j.1740-8709.2004.00001.x.
United Nations, 2008. United nations children’s fund: Progress for children: A report card on maternal mortality 2008 (7). UNICEF Division of Communication, New York. Available from www.unicef.org.
United Nations, 2008. United nations economic and social council- economic commission for Africa. First Joint Annual Meeting of African Union Ministers of Economic and Finance, and ECA Conference of African Ministers of Finance, Planning and Economic Development: Assessing progress in Africa towards the Millennium Development Goals Report.
World Health Organization, 2010. The department of making pregnancy safer, family and community health: Regional highlights 2009. Available from http://www.who.int/maternal_child_adolescent/documents/MPSProgressReport09-FINAL.pdf.
| Views and opinions expressed in this article are the views and opinions of the author(s), International Journal of Asian Social Science shall not be responsible or answerable for any loss, damage or liability etc. caused in relation to/arising out of the use of the content. |